S Prathyoosha, K Ananditha, T Narayana Rao, K V T Gopal, P V Krishnam Raju
{"title":"A Randomized Study to Evaluate the Efficacy of Oral Tranexamic Acid, Modified Kligman's Formula, and Placebo Cream in Melasma.","authors":"S Prathyoosha, K Ananditha, T Narayana Rao, K V T Gopal, P V Krishnam Raju","doi":"10.4103/idoj.idoj_797_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite the availability of various treatment modalities, the treatment of melasma is often incomplete, with a high recurrence rate. The present study was undertaken to assess the efficacy and safety of oral tranexamic acid (TXA), modified Kligman's formula (MKF), and a placebo cream in melasma.</p><p><strong>Materials and methods: </strong>Ninety cases of melasma of both sexes were enrolled, and divided into three groups of 30 patients each. The baseline severity of melasma was graded by Melasma Area Severity Index (MASI) score. Group A, B, and C patients were treated with oral TXA 250 mg twice daily, daily MKF cream at night, and daily placebo cream at night, respectively, for 12 weeks. Improvement in MASI score was calculated after 4, 8, and 12 weeks. At each visit, adverse effects, if any, were noted. Statistical analysis was done using Chi-square test.</p><p><strong>Results: </strong>Based on intention to treat analysis, at the end of 12 weeks, the reduction in MASI score in oral TXA, MKF, and placebo groups was 9.94(65.91%), 6.12(54.78%), and 2.07(17.22%), respectively (<i>P</i> = 0.00). The difference in reduction of mean MASI scores after 12 weeks between oral TXA group and MKF group was not significant (<i>P</i> = 0.29). The efficacy of oral TXA and MKB was significantly higher than that of the placebo group (<i>P</i> = 0.01 and <i>P</i> = 0.03, respectively). Adverse effects in all groups were mild and self-limiting.</p><p><strong>Limitations: </strong>A limited sample size, non-blinded design, and absence of dermoscopic evaluation were the study limitations.</p><p><strong>Conclusion: </strong>In view of its excellent safety profile, oral TXA may be considered as a better option for moderate to severe melasma.</p>","PeriodicalId":13335,"journal":{"name":"Indian Dermatology Online Journal","volume":"15 5","pages":"787-793"},"PeriodicalIF":2.0000,"publicationDate":"2024-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11444464/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Indian Dermatology Online Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/idoj.idoj_797_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Despite the availability of various treatment modalities, the treatment of melasma is often incomplete, with a high recurrence rate. The present study was undertaken to assess the efficacy and safety of oral tranexamic acid (TXA), modified Kligman's formula (MKF), and a placebo cream in melasma.
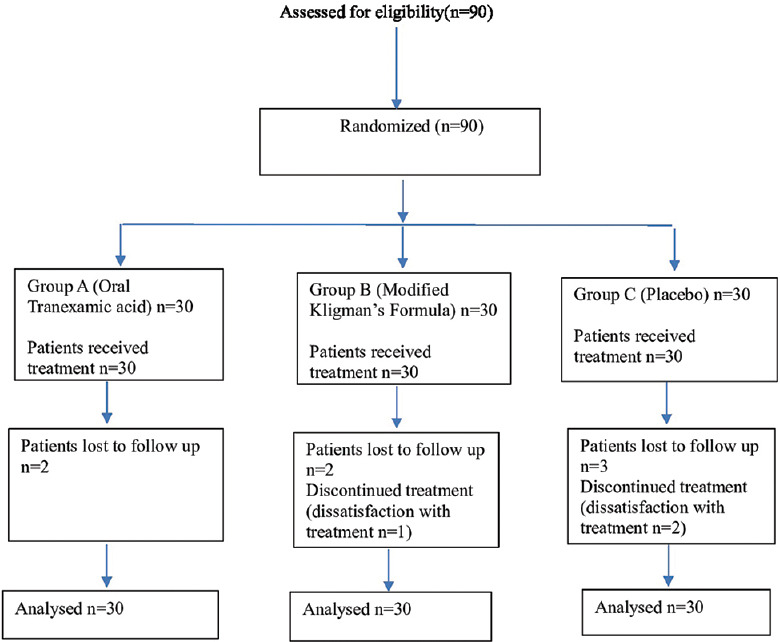
Materials and methods: Ninety cases of melasma of both sexes were enrolled, and divided into three groups of 30 patients each. The baseline severity of melasma was graded by Melasma Area Severity Index (MASI) score. Group A, B, and C patients were treated with oral TXA 250 mg twice daily, daily MKF cream at night, and daily placebo cream at night, respectively, for 12 weeks. Improvement in MASI score was calculated after 4, 8, and 12 weeks. At each visit, adverse effects, if any, were noted. Statistical analysis was done using Chi-square test.
Results: Based on intention to treat analysis, at the end of 12 weeks, the reduction in MASI score in oral TXA, MKF, and placebo groups was 9.94(65.91%), 6.12(54.78%), and 2.07(17.22%), respectively (P = 0.00). The difference in reduction of mean MASI scores after 12 weeks between oral TXA group and MKF group was not significant (P = 0.29). The efficacy of oral TXA and MKB was significantly higher than that of the placebo group (P = 0.01 and P = 0.03, respectively). Adverse effects in all groups were mild and self-limiting.
Limitations: A limited sample size, non-blinded design, and absence of dermoscopic evaluation were the study limitations.
Conclusion: In view of its excellent safety profile, oral TXA may be considered as a better option for moderate to severe melasma.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
