Jonny Currie, Kathrin Thomas, Anne M Cunningham, Kerry Bailey, Haroon Ahmed, Daniel Farewell, Sally Lewis
{"title":"Exploring the equity of distribution of general medical services funding allocations in Wales: a time-series analysis.","authors":"Jonny Currie, Kathrin Thomas, Anne M Cunningham, Kerry Bailey, Haroon Ahmed, Daniel Farewell, Sally Lewis","doi":"10.3399/BJGPO.2024.0080","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Good access to quality primary care in high-income countries can improve population health. Access to primary care is, however, often not equal among socioeconomic groups; our analysis sought to explore whether funding, a determinant of service supply, is equitably distributed among GP practices in Wales.</p><p><strong>Aim: </strong>To explore the relationship between funding and deprivation among GP practices in Wales, to understand the equity of current funding policies.</p><p><strong>Design & setting: </strong>A time-series analysis was undertaken in the primary care setting in Wales.</p><p><strong>Method: </strong>We obtained funding data for general practices in Wales between 2014 and 2022, and explored the equity of distribution using the percentage of practice patients living in the 20% most deprived small areas in Wales. We generated a linear regression model exploring the relationship between practice funding and deprivation, with an interaction term with time in years.</p><p><strong>Results: </strong>Practice funding rose for all practices between 2014 and 2022. Practice deprivation and time in years were both associated with practice funding, with increases in practice deprivation associated with reduced funding allocations, and time being associated with a small increase in funding over the study period. Over the period of analysis of 2014-2022, for every 10% increase in patients living in the most deprived lower layer super output areas, funding per patient decreased on average by 1%.</p><p><strong>Conclusion: </strong>General practices in Wales in more deprived areas receive discernibly less funding per patient than those in less deprived areas. Given the potential and likelihood primary care can affect population health outcomes, this underinvestment may be contributing to existing health inequalities and requires urgent further analysis and action.</p>","PeriodicalId":36541,"journal":{"name":"BJGP Open","volume":" ","pages":""},"PeriodicalIF":2.0000,"publicationDate":"2025-04-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12137987/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJGP Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3399/BJGPO.2024.0080","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Good access to quality primary care in high-income countries can improve population health. Access to primary care is, however, often not equal among socioeconomic groups; our analysis sought to explore whether funding, a determinant of service supply, is equitably distributed among GP practices in Wales.
Aim: To explore the relationship between funding and deprivation among GP practices in Wales, to understand the equity of current funding policies.
Design & setting: A time-series analysis was undertaken in the primary care setting in Wales.
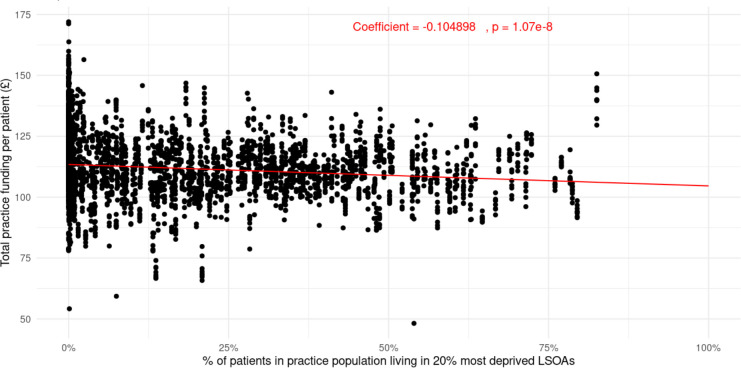
Method: We obtained funding data for general practices in Wales between 2014 and 2022, and explored the equity of distribution using the percentage of practice patients living in the 20% most deprived small areas in Wales. We generated a linear regression model exploring the relationship between practice funding and deprivation, with an interaction term with time in years.
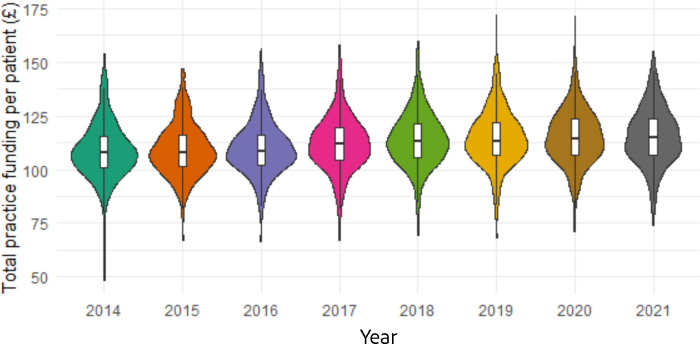
Results: Practice funding rose for all practices between 2014 and 2022. Practice deprivation and time in years were both associated with practice funding, with increases in practice deprivation associated with reduced funding allocations, and time being associated with a small increase in funding over the study period. Over the period of analysis of 2014-2022, for every 10% increase in patients living in the most deprived lower layer super output areas, funding per patient decreased on average by 1%.
Conclusion: General practices in Wales in more deprived areas receive discernibly less funding per patient than those in less deprived areas. Given the potential and likelihood primary care can affect population health outcomes, this underinvestment may be contributing to existing health inequalities and requires urgent further analysis and action.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
