{"title":"Smoking Status and Premature Death Among Japanese Rural Community-Dwelling Persons.","authors":"Ryuichi Kawamoto, Asuka Kikuchi, Daisuke Ninomiya, Masanori Abe, Teru Kumagi","doi":"10.1177/1179173X241275881","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Smoking status is known to be an independent and significant predictor of health outcomes related to aging and plays a crucial role in overall mortality rates. This cohort study investigated the relationship between smoking status and survival outcomes over follow-up periods of 9 and 21 years. <b>Methods:</b> The sample consisted of 3526 participants with a mean age of 64 ± 12 years, 44.1% of whom were male. The median follow-up duration was 6315 days, with an interquartile range of 3441 to 7727 days. Smoking status [i.e., Brinkmann index (BI)] was calculated by multiplying the number of years smoked by the number of cigarettes smoked daily. Based on this, participants were categorized into non-smokers, former smokers, and current smokers. The data were analyzed using Cox regression, employing age as the time variable and accounting for various risk factors. <b>Results:</b> A total of 1111 participants (49.2%) were confirmed to have died. Among these, 564 were male (36.2% of all male participants), and 547 were female (27.8% of all female participants). The multivariate-adjusted odds ratio (95% confidence interval) for all-cause mortality compared with never-smokers was 1.51 (1.17-1.96) for former smokers with BI > 800, 1.61 (1.20-2.17) for current smokers with BI of 400-799 and 1.62 (95% CI, 1.24-2.10) with BI of ≥800 (<i>P</i> for trend <0.001). Participants who died within three years of follow-up were excluded to avoid the possibility of reverse causation, but the results were essentially unchanged. <b>Conclusion:</b> We found that the BI is a valid predictor of future mortality risk and that BI 800 for former smokers and BI 400 for current smokers were useful cutoff values. Efforts to control smoking should focus not only on current smokers but also on former smokers to reduce the risk of premature death associated with smoking.</p>","PeriodicalId":43361,"journal":{"name":"Tobacco Use Insights","volume":"17 ","pages":"1179173X241275881"},"PeriodicalIF":2.1000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11447718/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tobacco Use Insights","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179173X241275881","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
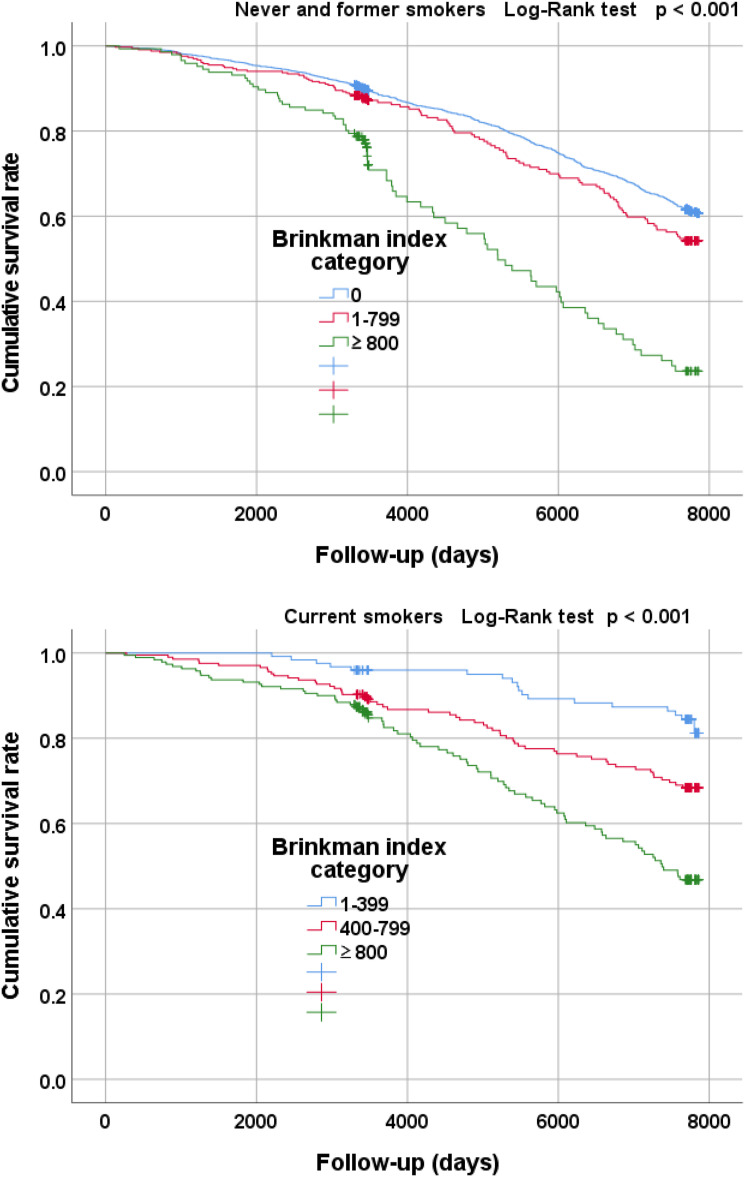
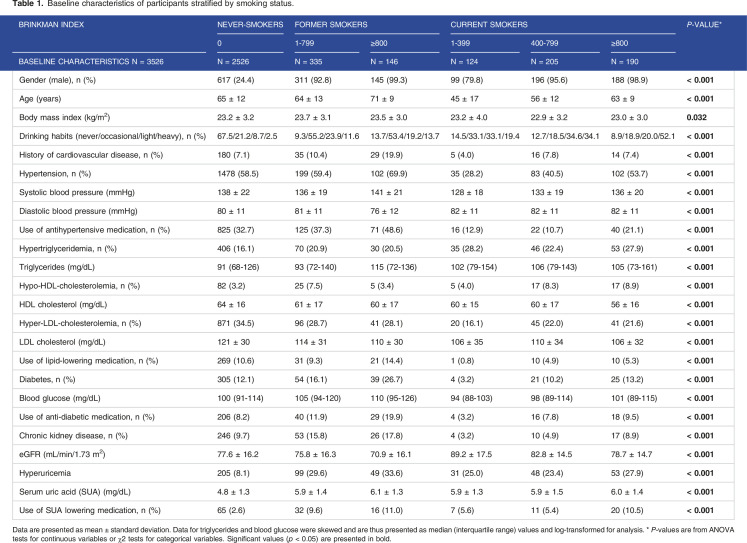
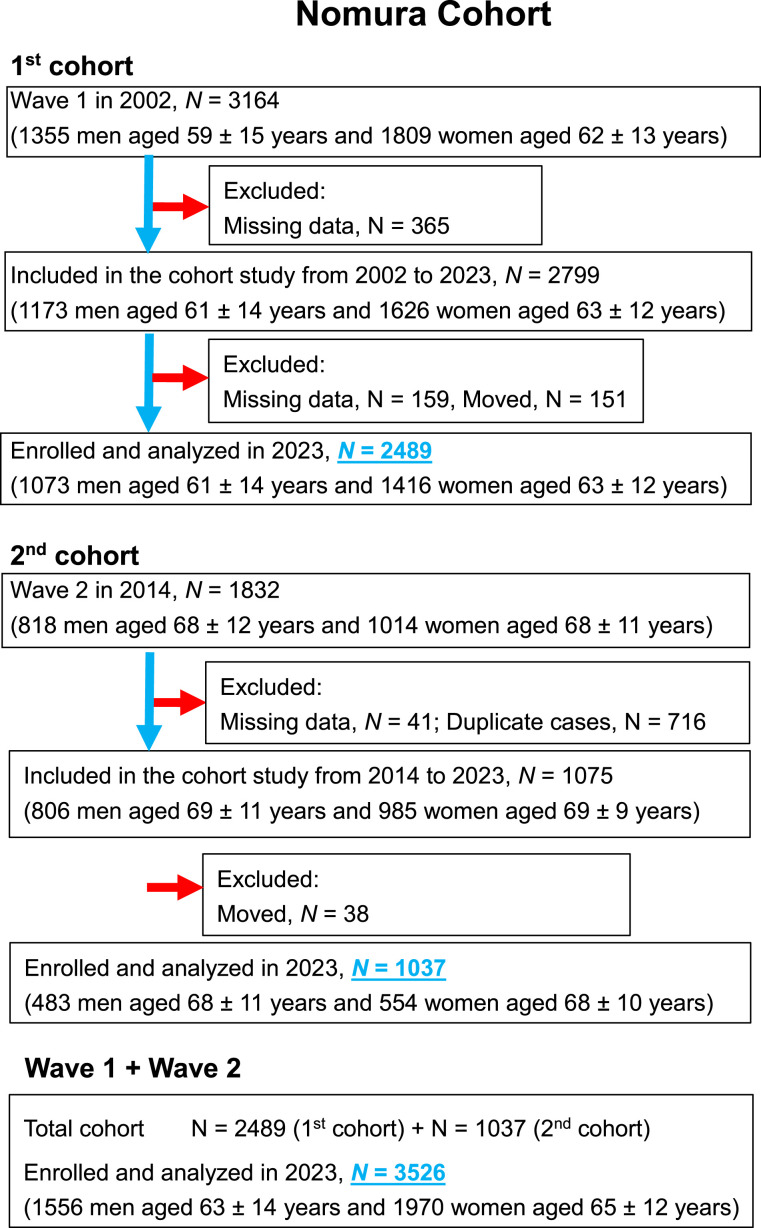
Background: Smoking status is known to be an independent and significant predictor of health outcomes related to aging and plays a crucial role in overall mortality rates. This cohort study investigated the relationship between smoking status and survival outcomes over follow-up periods of 9 and 21 years. Methods: The sample consisted of 3526 participants with a mean age of 64 ± 12 years, 44.1% of whom were male. The median follow-up duration was 6315 days, with an interquartile range of 3441 to 7727 days. Smoking status [i.e., Brinkmann index (BI)] was calculated by multiplying the number of years smoked by the number of cigarettes smoked daily. Based on this, participants were categorized into non-smokers, former smokers, and current smokers. The data were analyzed using Cox regression, employing age as the time variable and accounting for various risk factors. Results: A total of 1111 participants (49.2%) were confirmed to have died. Among these, 564 were male (36.2% of all male participants), and 547 were female (27.8% of all female participants). The multivariate-adjusted odds ratio (95% confidence interval) for all-cause mortality compared with never-smokers was 1.51 (1.17-1.96) for former smokers with BI > 800, 1.61 (1.20-2.17) for current smokers with BI of 400-799 and 1.62 (95% CI, 1.24-2.10) with BI of ≥800 (P for trend <0.001). Participants who died within three years of follow-up were excluded to avoid the possibility of reverse causation, but the results were essentially unchanged. Conclusion: We found that the BI is a valid predictor of future mortality risk and that BI 800 for former smokers and BI 400 for current smokers were useful cutoff values. Efforts to control smoking should focus not only on current smokers but also on former smokers to reduce the risk of premature death associated with smoking.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
