Daniel Mashiach, Patrice Mead, Kendall Carneiro, Jemily Malvar, Susan Knight, Guy Young
{"title":"CHIEF: A retrospective self-control study of children with severe hemophilia A without inhibitors comparing emicizumab to FVIII prophylaxis","authors":"Daniel Mashiach, Patrice Mead, Kendall Carneiro, Jemily Malvar, Susan Knight, Guy Young","doi":"10.1002/pbc.31351","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Hemophilia A (HA) is an X-linked bleeding disorder diagnosed by a deficiency in factor VIII (FVIII). For severe HA (SHA), prophylaxis clotting factor concentrates (CFC) has become the standard of care; however, it imparts a high treatment burden and typically results in an annualized bleeding rate (ABR) of 2–6. Emicizumab, a subcutaneously administered FVIII substitute, has become the de facto standard-of-care prophylaxis for children with SHA in many countries. Previous clinical trials of emicizumab have assessed ABR in patients greater than 12 years without inhibitors, and in children less than 12 years with inhibitors; however, there is little information published regarding the ABR of emicizumab compared to CFC in non-inhibitor SHA children.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Using a retrospective electronic medical record chart review, we conducted a self-control analysis of 15 patients less than 12 years of age during equivalent periods of CFC versus emicizumab prophylaxis.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The mean ABR on CFC and emicizumab was 1.79 and 1.13 (<i>p</i> = .092), respectively, with a substantially decreased rate of joint bleeds (CFC 0.94; emicizumab 0.33; <i>p</i> = .001) and spontaneous bleeds (CFC 0.79; emicizumab 0.23; <i>p</i> = .008). No safety events were recorded for patients while administering emicizumab. The mean annual cost of CFC prophylaxis was $515,340 (SD $199,540), compared to $328,410 (SD $137,230) for emicizumab prophylaxis (<i>p</i> < .001).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Emicizumab resulted in an improved ABR compared to CFC, especially for joint and spontaneous bleeds, had fewer administration complications, and was substantially less expensive compared to CFC prophylaxis; however, more research is necessary for a complete understanding of the effect of emicizumab on joint health and muscle bleeds.</p>\n </section>\n </div>","PeriodicalId":19822,"journal":{"name":"Pediatric Blood & Cancer","volume":"71 12","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2024-10-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/pbc.31351","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Blood & Cancer","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/pbc.31351","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Hemophilia A (HA) is an X-linked bleeding disorder diagnosed by a deficiency in factor VIII (FVIII). For severe HA (SHA), prophylaxis clotting factor concentrates (CFC) has become the standard of care; however, it imparts a high treatment burden and typically results in an annualized bleeding rate (ABR) of 2–6. Emicizumab, a subcutaneously administered FVIII substitute, has become the de facto standard-of-care prophylaxis for children with SHA in many countries. Previous clinical trials of emicizumab have assessed ABR in patients greater than 12 years without inhibitors, and in children less than 12 years with inhibitors; however, there is little information published regarding the ABR of emicizumab compared to CFC in non-inhibitor SHA children.
Methods
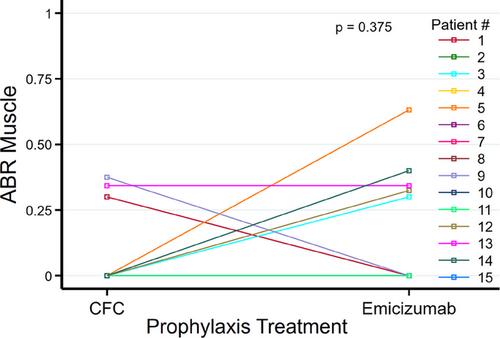
Using a retrospective electronic medical record chart review, we conducted a self-control analysis of 15 patients less than 12 years of age during equivalent periods of CFC versus emicizumab prophylaxis.
Results
The mean ABR on CFC and emicizumab was 1.79 and 1.13 (p = .092), respectively, with a substantially decreased rate of joint bleeds (CFC 0.94; emicizumab 0.33; p = .001) and spontaneous bleeds (CFC 0.79; emicizumab 0.23; p = .008). No safety events were recorded for patients while administering emicizumab. The mean annual cost of CFC prophylaxis was $515,340 (SD $199,540), compared to $328,410 (SD $137,230) for emicizumab prophylaxis (p < .001).
Conclusion
Emicizumab resulted in an improved ABR compared to CFC, especially for joint and spontaneous bleeds, had fewer administration complications, and was substantially less expensive compared to CFC prophylaxis; however, more research is necessary for a complete understanding of the effect of emicizumab on joint health and muscle bleeds.
期刊介绍:
Pediatric Blood & Cancer publishes the highest quality manuscripts describing basic and clinical investigations of blood disorders and malignant diseases of childhood including diagnosis, treatment, epidemiology, etiology, biology, and molecular and clinical genetics of these diseases as they affect children, adolescents, and young adults. Pediatric Blood & Cancer will also include studies on such treatment options as hematopoietic stem cell transplantation, immunology, and gene therapy.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
