Gagan Priya, Bashir A Laway, Mythili Ayyagari, Milinda Gupta, Ganesh H K Bhat, Deep Dutta
{"title":"The Glucocorticoid Taper: A Primer for the Clinicians.","authors":"Gagan Priya, Bashir A Laway, Mythili Ayyagari, Milinda Gupta, Ganesh H K Bhat, Deep Dutta","doi":"10.4103/ijem.ijem_410_23","DOIUrl":null,"url":null,"abstract":"<p><p>Glucocorticoid (GC) therapy can ameliorate debilitating and life-threatening symptoms in several inflammatory/immunological disorders. However, it can also cause significant side effects, especially with higher doses and longer duration of use. Therefore, GCs should be used at the lowest effective dose for the shortest possible time to minimise adverse effects. GC therapy may cause suppression of the endogenous hypothalamic-pituitary-adrenal (HPA) axis and abrupt discontinuation predisposes patients to features of GC-induced adrenal insufficiency. The practice of tapering GC therapy allows for recovery of the HPA axis while minimising the risk of a disease flare-up or symptoms of AI. Moderate-to-high dose GC therapy may be tapered rapidly to near-physiological doses while watching for features of disease reactivation. Once close to the physiological dose, tapering is slower and at longer intervals to allow for recovery of the HPA axis. It is important to use short- or intermediate-acting GC preparations such as hydrocortisone or prednisolone in physiological doses, administered in the morning to mimic the endogenous cortisol rhythm. A general principle to follow is that HPA axis recovery takes longer if the period of suppression has been long. In such cases, tapering should be slower over a few months to even a year. In select cases at high risk of AI or if symptoms appear during tapering, the decision to further taper and discontinue steroids may be based on testing of HPA axis function using basal and/or stimulated serum cortisol. All patients on exogenous steroids should be advised about the need for an appropriate increase in GC doses during acute medical or surgical illness and should carry a steroid alert card to avoid adrenal crisis.</p>","PeriodicalId":13353,"journal":{"name":"Indian Journal of Endocrinology and Metabolism","volume":"28 4","pages":"350-362"},"PeriodicalIF":0.0000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11451960/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Indian Journal of Endocrinology and Metabolism","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/ijem.ijem_410_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/28 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
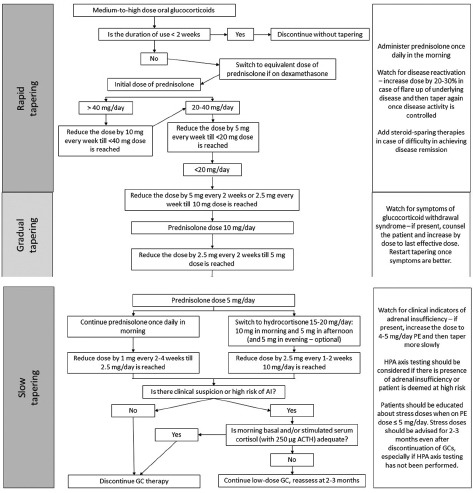
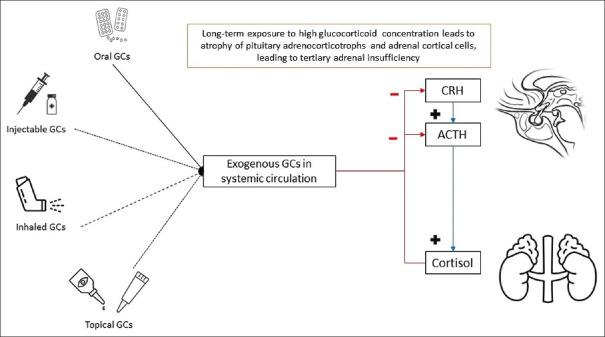
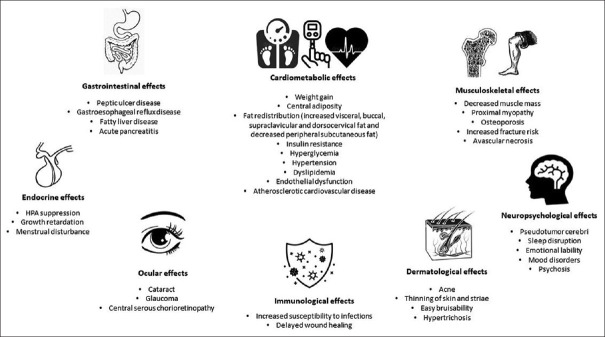
Glucocorticoid (GC) therapy can ameliorate debilitating and life-threatening symptoms in several inflammatory/immunological disorders. However, it can also cause significant side effects, especially with higher doses and longer duration of use. Therefore, GCs should be used at the lowest effective dose for the shortest possible time to minimise adverse effects. GC therapy may cause suppression of the endogenous hypothalamic-pituitary-adrenal (HPA) axis and abrupt discontinuation predisposes patients to features of GC-induced adrenal insufficiency. The practice of tapering GC therapy allows for recovery of the HPA axis while minimising the risk of a disease flare-up or symptoms of AI. Moderate-to-high dose GC therapy may be tapered rapidly to near-physiological doses while watching for features of disease reactivation. Once close to the physiological dose, tapering is slower and at longer intervals to allow for recovery of the HPA axis. It is important to use short- or intermediate-acting GC preparations such as hydrocortisone or prednisolone in physiological doses, administered in the morning to mimic the endogenous cortisol rhythm. A general principle to follow is that HPA axis recovery takes longer if the period of suppression has been long. In such cases, tapering should be slower over a few months to even a year. In select cases at high risk of AI or if symptoms appear during tapering, the decision to further taper and discontinue steroids may be based on testing of HPA axis function using basal and/or stimulated serum cortisol. All patients on exogenous steroids should be advised about the need for an appropriate increase in GC doses during acute medical or surgical illness and should carry a steroid alert card to avoid adrenal crisis.
期刊介绍:
The Indian Journal of Endocrinology and Metabolism (IJEM) aims to function as the global face of Indian endocrinology research. It aims to act as a bridge between global and national advances in this field. The journal publishes thought-provoking editorials, comprehensive reviews, cutting-edge original research, focused brief communications and insightful letters to editor. The journal encourages authors to submit articles addressing aspects of science related to Endocrinology and Metabolism in particular Diabetology. Articles related to Clinical and Tropical endocrinology are especially encouraged. Sub-topic based Supplements are published regularly. This allows the journal to highlight issues relevant to Endocrine practitioners working in India as well as other countries. IJEM is free access in the true sense of the word, (it charges neither authors nor readers) and this enhances its global appeal.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
