Systemic amyloidosis: an aggressive evolution in a patient with relapsing polychondritis and monoclonal gammopathy of undetermined significance (MGUS) undergoing peritoneal dialysis.
Thiago Cavalcanti Matos, William George Giusti Fischer, Rosa Maria Rodrigues Pereira, Andre Silva Franco
{"title":"Systemic amyloidosis: an aggressive evolution in a patient with relapsing polychondritis and monoclonal gammopathy of undetermined significance (MGUS) undergoing peritoneal dialysis.","authors":"Thiago Cavalcanti Matos, William George Giusti Fischer, Rosa Maria Rodrigues Pereira, Andre Silva Franco","doi":"10.4322/acr.2024.518","DOIUrl":null,"url":null,"abstract":"<p><p>Herein, we report the case of primary amyloidosis with multi-organ involvement in a female patient in her 50s. The patient had a history of relapsing polychondritis, chronic kidney disease, and monoclonal gammopathy of undetermined significance (MGUS). The clinical manifestations included neuropathic pain, sensorimotor polyneuropathy, intrahepatic cholestatic liver injury, gastrointestinal symptoms, dysautonomia, and myocardial thickening. Initial histologic evaluations of the abdominal fat pad aspirate and bone marrow biopsy were negative for amyloid deposition. However, due to a high index of suspicion, a second bone marrow biopsy was performed, confirming the presence of the amyloid protein. Given the patient's complex medical history, other types of amyloidosis, such as AA amyloidosis, AL amyloidosis, and ß2-microglobulin amyloidosis, should also be considered as differential diagnoses. The type of amyloid protein was subsequently identified through laser microdissection of amyloid fibrils followed by liquid chromatography-tandem mass spectrometry as AL-lambda (amyloid light-chain) amyloidosis. The patient presented unfavorable evolution, with progressive dysautonomia, being admitted to the ICU, culminating in refractory circulatory shock, and undergoing an empirical broad-spectrum antibiotic therapy. After a few days, she presented pulseless ventricular tachycardia, culminating in her death, before undergoing specific treatment. This article highlights the crucial role of precise identification in guiding appropriate therapeutic strategies for this complex, yet potentially severe, diseases.</p>","PeriodicalId":53117,"journal":{"name":"Autopsy and Case Reports","volume":"14 ","pages":"e2024518"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11452076/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Autopsy and Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4322/acr.2024.518","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
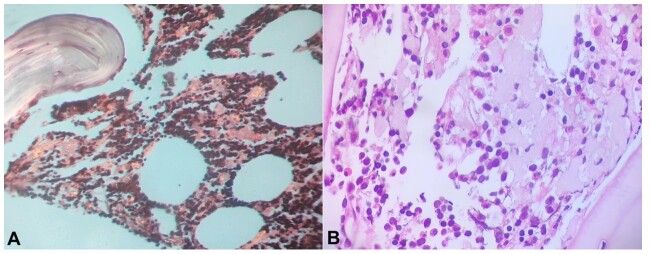
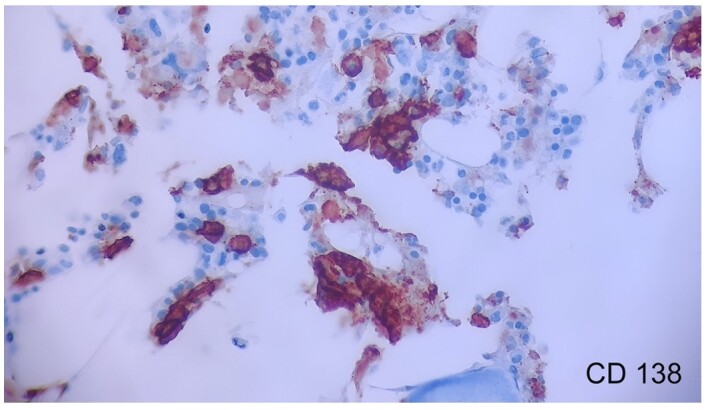
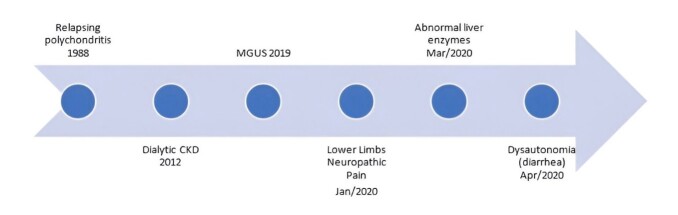
Herein, we report the case of primary amyloidosis with multi-organ involvement in a female patient in her 50s. The patient had a history of relapsing polychondritis, chronic kidney disease, and monoclonal gammopathy of undetermined significance (MGUS). The clinical manifestations included neuropathic pain, sensorimotor polyneuropathy, intrahepatic cholestatic liver injury, gastrointestinal symptoms, dysautonomia, and myocardial thickening. Initial histologic evaluations of the abdominal fat pad aspirate and bone marrow biopsy were negative for amyloid deposition. However, due to a high index of suspicion, a second bone marrow biopsy was performed, confirming the presence of the amyloid protein. Given the patient's complex medical history, other types of amyloidosis, such as AA amyloidosis, AL amyloidosis, and ß2-microglobulin amyloidosis, should also be considered as differential diagnoses. The type of amyloid protein was subsequently identified through laser microdissection of amyloid fibrils followed by liquid chromatography-tandem mass spectrometry as AL-lambda (amyloid light-chain) amyloidosis. The patient presented unfavorable evolution, with progressive dysautonomia, being admitted to the ICU, culminating in refractory circulatory shock, and undergoing an empirical broad-spectrum antibiotic therapy. After a few days, she presented pulseless ventricular tachycardia, culminating in her death, before undergoing specific treatment. This article highlights the crucial role of precise identification in guiding appropriate therapeutic strategies for this complex, yet potentially severe, diseases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
