Daina Kashiwazaki, Shusuke Yamamoto, Emiko Hori, Naoki Akioka, Kyo Noguchi, Satoshi Kuroda
{"title":"Reversible sulcal fluid-attenuated inversion recovery hyperintensity after combined bypass surgery for moyamoya disease - A \"crevasse\" sign.","authors":"Daina Kashiwazaki, Shusuke Yamamoto, Emiko Hori, Naoki Akioka, Kyo Noguchi, Satoshi Kuroda","doi":"10.25259/SNI_571_2024","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Transient fluid-attenuated inversion recovery (FLAIR) hyperintensity is often observed on the operated brain surface after direct or combined bypass surgery for moyamoya disease, but its pathophysiology and clinical significance are still obscure. This study was aimed to clarify the underlying mechanism and clinical significance.</p><p><strong>Methods: </strong>This prospective study included 106 hemispheres of 61 patients with moyamoya disease and analyzed their radiological findings before and after combined bypass surgery. This study also included 11 patients who underwent superficial temporal artery to middle cerebral artery anastomosis for occlusive carotid artery diseases as the controls. Magnetic resonance imaging examination was serially repeated, and cerebral blood flow was measured before and after surgery. Signal intensity ratio (SIR) in the cortical sulci and cortex to the adjacent white matter on FLAIR images was calculated, and the postoperative SIR changes were semi-quantitatively evaluated to assess the temporal profile of postoperative FLAIR hyperintensity.</p><p><strong>Results: </strong>Postoperative FLAIR hyperintensity occurred within the cortical sulci on the operated hemispheres in all moyamoya patients but not in patients with occlusive carotid artery diseases. SIR values started to increase immediately after surgery, peaked at about 4-fold at 4-13 days post-surgery, then declined, and recovered to baseline values over 28 days or later. The magnitude of this phenomenon was proportional to the severity of cerebral ischemia but not to postoperative hyperperfusion.</p><p><strong>Conclusion: </strong>Reversible sulcal FLAIR hyperintensity specifically occurs in the operated hemispheres after direct bypass surgery for moyamoya disease. This \"<i>crevasse sign</i>\" may represent the mixture of the extensive leakage of oxygen and proteins from the pial arteries into the CSF.</p>","PeriodicalId":94217,"journal":{"name":"Surgical neurology international","volume":"15 ","pages":"322"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11450489/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical neurology international","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.25259/SNI_571_2024","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Transient fluid-attenuated inversion recovery (FLAIR) hyperintensity is often observed on the operated brain surface after direct or combined bypass surgery for moyamoya disease, but its pathophysiology and clinical significance are still obscure. This study was aimed to clarify the underlying mechanism and clinical significance.
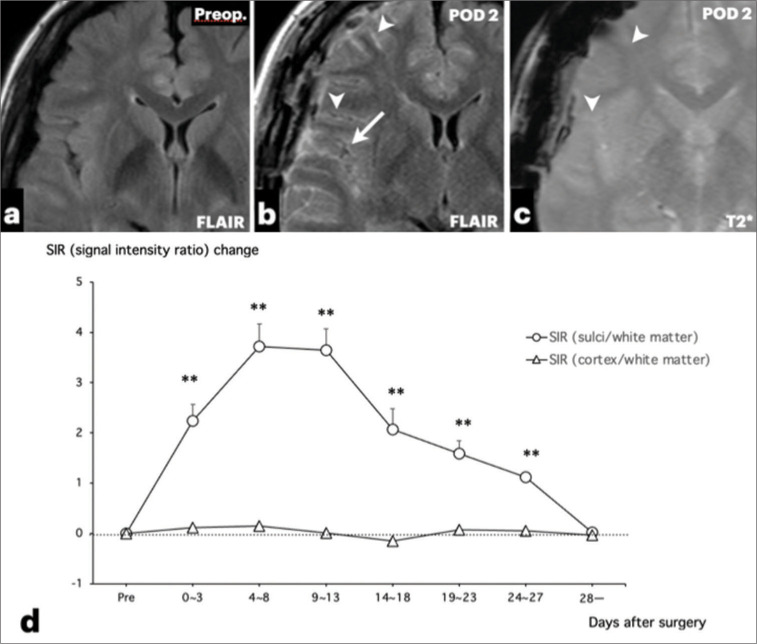
Methods: This prospective study included 106 hemispheres of 61 patients with moyamoya disease and analyzed their radiological findings before and after combined bypass surgery. This study also included 11 patients who underwent superficial temporal artery to middle cerebral artery anastomosis for occlusive carotid artery diseases as the controls. Magnetic resonance imaging examination was serially repeated, and cerebral blood flow was measured before and after surgery. Signal intensity ratio (SIR) in the cortical sulci and cortex to the adjacent white matter on FLAIR images was calculated, and the postoperative SIR changes were semi-quantitatively evaluated to assess the temporal profile of postoperative FLAIR hyperintensity.
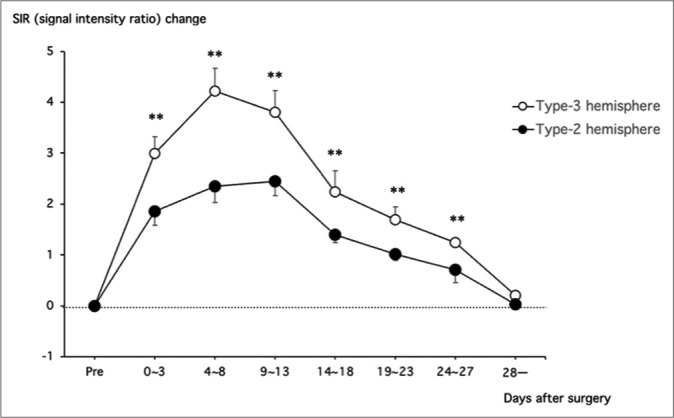
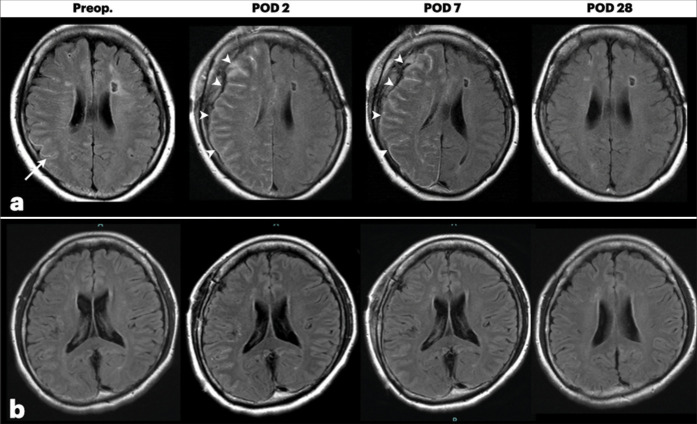
Results: Postoperative FLAIR hyperintensity occurred within the cortical sulci on the operated hemispheres in all moyamoya patients but not in patients with occlusive carotid artery diseases. SIR values started to increase immediately after surgery, peaked at about 4-fold at 4-13 days post-surgery, then declined, and recovered to baseline values over 28 days or later. The magnitude of this phenomenon was proportional to the severity of cerebral ischemia but not to postoperative hyperperfusion.
Conclusion: Reversible sulcal FLAIR hyperintensity specifically occurs in the operated hemispheres after direct bypass surgery for moyamoya disease. This "crevasse sign" may represent the mixture of the extensive leakage of oxygen and proteins from the pial arteries into the CSF.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
