Benjamin A. Derman, Ajay Major, Jennifer Cooperrider, Ken Jiang, Aubrianna Ramsland, Theodore Karrison, Tadeusz Kubicki, Andrzej J. Jakubowiak
{"title":"Discontinuation of maintenance therapy in multiple myeloma guided by multimodal measurable residual disease negativity (MRD2STOP)","authors":"Benjamin A. Derman, Ajay Major, Jennifer Cooperrider, Ken Jiang, Aubrianna Ramsland, Theodore Karrison, Tadeusz Kubicki, Andrzej J. Jakubowiak","doi":"10.1038/s41408-024-01156-x","DOIUrl":null,"url":null,"abstract":"<p>MRD2STOP is a pragmatic trial evaluating maintenance therapy cessation guided by measurable residual disease (MRD) negativity in multiple myeloma (MM). Eligible patients had previous MRD < 10<sup>−5</sup>, received ≥1 year of maintenance, and were prospectively confirmed to have undetectable disease by positron emission tomography, bone marrow (BM) flow cytometry (limit of detection [LoD] 10<sup>−</sup><sup>5</sup>), and BM clonoSEQ (LoD 10<sup>−</sup><sup>6</sup>). BM aspirates enriched for CD138<sup>+</sup> cells were analyzed by clonoSEQ to achieve MRD 10<sup>−</sup><sup>7</sup> sensitivity. We evaluated the incidence of disease resurgence and progression-free survival (PFS), stratified by 10<sup>−</sup><sup>7</sup> status. Forty-seven patients discontinued maintenance after a median of 36 months. Baseline MRD ≥ 10<sup>−</sup><sup>7</sup> was observed in 19% (9/47). The median follow-up post-discontinuation was 30 months. Disease resurgence (MRD 10 ≥ <sup>−</sup><sup>6</sup>) occurred in 11 patients, including 5 disease progressions. One patient died from a second cancer. The estimated 3-year cumulative incidence of disease resurgence was 20% for patients with baseline MRD < 10<sup>−</sup><sup>7</sup> compared to 75% for MRD ≥ 10<sup>−</sup><sup>7</sup> (HR 7.8, 95% CI 2.2-27.6, p = 0.001). Baseline MRD ≥ 10<sup>−</sup><sup>7</sup> was associated with inferior PFS compared to MRD < 10<sup>−</sup><sup>7</sup> (HR 10.1, 95% CI 1.6–62.3; 3-year PFS 49% vs 92%). Maintenance discontinuation in patients with MM and MRD < 10<sup>−</sup><sup>6</sup> led to low rates of disease resurgence. MRD < 10<sup>−</sup><sup>7</sup> may be a superior cessation threshold, requiring further validation.</p><figure></figure>","PeriodicalId":8989,"journal":{"name":"Blood Cancer Journal","volume":"12 1","pages":""},"PeriodicalIF":11.6000,"publicationDate":"2024-10-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood Cancer Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41408-024-01156-x","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
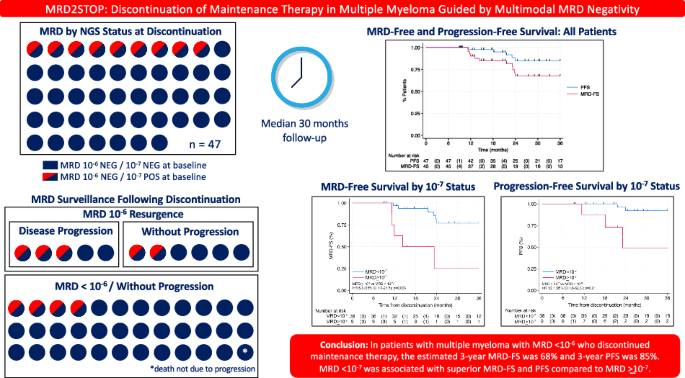
MRD2STOP is a pragmatic trial evaluating maintenance therapy cessation guided by measurable residual disease (MRD) negativity in multiple myeloma (MM). Eligible patients had previous MRD < 10−5, received ≥1 year of maintenance, and were prospectively confirmed to have undetectable disease by positron emission tomography, bone marrow (BM) flow cytometry (limit of detection [LoD] 10−5), and BM clonoSEQ (LoD 10−6). BM aspirates enriched for CD138+ cells were analyzed by clonoSEQ to achieve MRD 10−7 sensitivity. We evaluated the incidence of disease resurgence and progression-free survival (PFS), stratified by 10−7 status. Forty-seven patients discontinued maintenance after a median of 36 months. Baseline MRD ≥ 10−7 was observed in 19% (9/47). The median follow-up post-discontinuation was 30 months. Disease resurgence (MRD 10 ≥ −6) occurred in 11 patients, including 5 disease progressions. One patient died from a second cancer. The estimated 3-year cumulative incidence of disease resurgence was 20% for patients with baseline MRD < 10−7 compared to 75% for MRD ≥ 10−7 (HR 7.8, 95% CI 2.2-27.6, p = 0.001). Baseline MRD ≥ 10−7 was associated with inferior PFS compared to MRD < 10−7 (HR 10.1, 95% CI 1.6–62.3; 3-year PFS 49% vs 92%). Maintenance discontinuation in patients with MM and MRD < 10−6 led to low rates of disease resurgence. MRD < 10−7 may be a superior cessation threshold, requiring further validation.
期刊介绍:
Blood Cancer Journal is dedicated to publishing high-quality articles related to hematologic malignancies and related disorders. The journal welcomes submissions of original research, reviews, guidelines, and letters that are deemed to have a significant impact in the field. While the journal covers a wide range of topics, it particularly focuses on areas such as:
Preclinical studies of new compounds, especially those that provide mechanistic insights
Clinical trials and observations
Reviews related to new drugs and current management of hematologic malignancies
Novel observations related to new mutations, molecular pathways, and tumor genomics
Blood Cancer Journal offers a forum for expedited publication of novel observations regarding new mutations or altered pathways.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
