Kerstine Carter, Olga Kuznetsova, Volodymyr Anisimov, Johannes Krisam, Colin Scherer, Yevgen Ryeznik, Oleksandr Sverdlov
{"title":"Forced randomization: the what, why, and how.","authors":"Kerstine Carter, Olga Kuznetsova, Volodymyr Anisimov, Johannes Krisam, Colin Scherer, Yevgen Ryeznik, Oleksandr Sverdlov","doi":"10.1186/s12874-024-02340-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>When running a randomized controlled trial (RCT), a clinical site may face a situation when an eligible trial participant is to be randomized to the treatment that is not available at the site. In this case, there are two options: not to enroll the participant, or, without disclosing to the site, allocate the participant to a treatment arm with drug available at the site using a built-in feature of the interactive response technology (IRT). In the latter case, one has employed a \"forced randomization\" (FR). There seems to be an industry-wide consensus that using FR can be acceptable in confirmatory trials provided there are \"not too many\" instances of forcing. A better understanding of statistical properties of FR is warranted.</p><p><strong>Methods: </strong>We described four different IRT configurations with or without FR and illustrated them using a simple example. We discussed potential merits of FR and outlined some relevant theoretical risks and risk mitigation strategies. We performed a search using Cortellis Regulatory Intelligence database (IDRAC) ( www.cortellis.com ) to understand the prevalence of FR in clinical trial practice. We also proposed a structured template for development and evaluation of randomization designs featuring FR and showcased an application of this template for a hypothetical multi-center 1:1 RCT under three experimental settings (\"base case\", \"slower recruitment\", and \"faster recruitment\") to explore the effect of four different IRT configurations in combination with three different drug supply/re-supply strategies on some important operating characteristics of the trial. We also supplied the Julia code that can be used to reproduce our simulation results and generate additional results under user-specified experimental scenarios.</p><p><strong>Results: </strong>FR can eliminate refusals to randomize patients, which can cause frustration for patients and study site personnel, improve the study logistics, drug supply management, cost-efficiency, and recruitment time. Nevertheless, FR carries some potential risks that should be reviewed at the study planning stage and, ideally, prospectively addressed through risk mitigation planning. The Cortellis search identified only 9 submissions that have reported the use of FR; typically, the FR option was documented in IRT specifications. Our simulation evidence showed that under the considered realistic experimental settings, the percentage of FR is expected to be low. When FR with backfilling was used in combination with high re-supply strategy, the final treatment imbalance was negligibly small, the proportion of patients not randomized due to the lack of drug supply was close to zero, and the time to complete recruitment was shortened compared to the case when FR was not allowed. The drug overage was primarily determined by the intensity of the re-supply strategy and to a smaller extent by the presence or absence of the FR feature in IRT.</p><p><strong>Conclusion: </strong>FR with a carefully chosen drug supply/re-supply strategy can result in quantifiable improvements in the patients' and site personnel experience, trial logistics and efficiency while preventing an undesirable refusal to randomize a patient and a consequential unblinding at the site. FR is a useful design feature of multi-center RCTs provided it is properly planned for and carefully implemented.</p>","PeriodicalId":9114,"journal":{"name":"BMC Medical Research Methodology","volume":"24 1","pages":"234"},"PeriodicalIF":3.4000,"publicationDate":"2024-10-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11459895/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Medical Research Methodology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12874-024-02340-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: When running a randomized controlled trial (RCT), a clinical site may face a situation when an eligible trial participant is to be randomized to the treatment that is not available at the site. In this case, there are two options: not to enroll the participant, or, without disclosing to the site, allocate the participant to a treatment arm with drug available at the site using a built-in feature of the interactive response technology (IRT). In the latter case, one has employed a "forced randomization" (FR). There seems to be an industry-wide consensus that using FR can be acceptable in confirmatory trials provided there are "not too many" instances of forcing. A better understanding of statistical properties of FR is warranted.
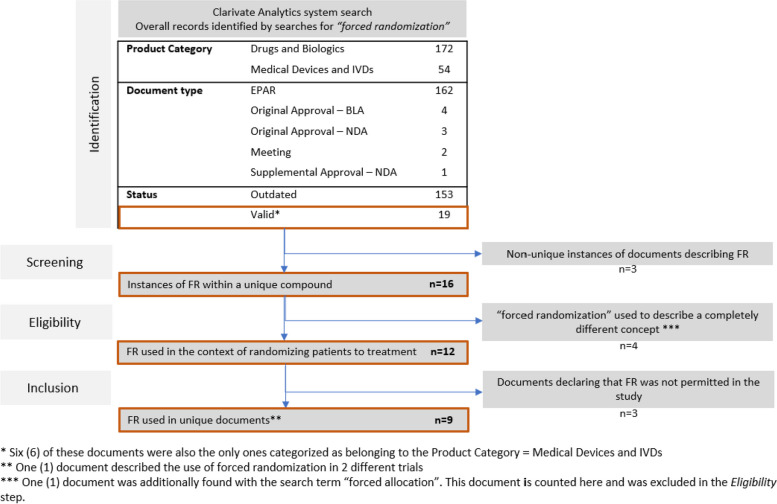
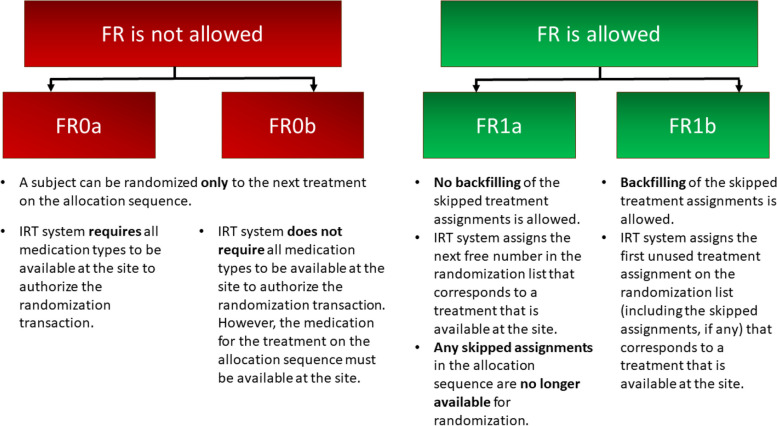
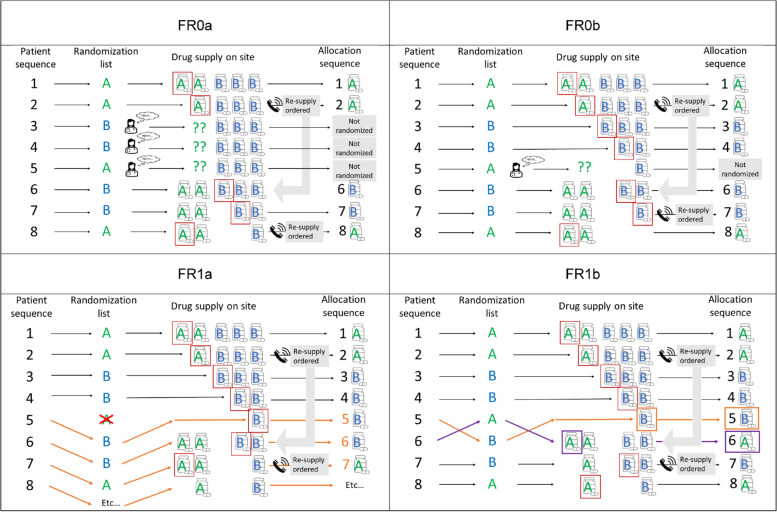
Methods: We described four different IRT configurations with or without FR and illustrated them using a simple example. We discussed potential merits of FR and outlined some relevant theoretical risks and risk mitigation strategies. We performed a search using Cortellis Regulatory Intelligence database (IDRAC) ( www.cortellis.com ) to understand the prevalence of FR in clinical trial practice. We also proposed a structured template for development and evaluation of randomization designs featuring FR and showcased an application of this template for a hypothetical multi-center 1:1 RCT under three experimental settings ("base case", "slower recruitment", and "faster recruitment") to explore the effect of four different IRT configurations in combination with three different drug supply/re-supply strategies on some important operating characteristics of the trial. We also supplied the Julia code that can be used to reproduce our simulation results and generate additional results under user-specified experimental scenarios.
Results: FR can eliminate refusals to randomize patients, which can cause frustration for patients and study site personnel, improve the study logistics, drug supply management, cost-efficiency, and recruitment time. Nevertheless, FR carries some potential risks that should be reviewed at the study planning stage and, ideally, prospectively addressed through risk mitigation planning. The Cortellis search identified only 9 submissions that have reported the use of FR; typically, the FR option was documented in IRT specifications. Our simulation evidence showed that under the considered realistic experimental settings, the percentage of FR is expected to be low. When FR with backfilling was used in combination with high re-supply strategy, the final treatment imbalance was negligibly small, the proportion of patients not randomized due to the lack of drug supply was close to zero, and the time to complete recruitment was shortened compared to the case when FR was not allowed. The drug overage was primarily determined by the intensity of the re-supply strategy and to a smaller extent by the presence or absence of the FR feature in IRT.
Conclusion: FR with a carefully chosen drug supply/re-supply strategy can result in quantifiable improvements in the patients' and site personnel experience, trial logistics and efficiency while preventing an undesirable refusal to randomize a patient and a consequential unblinding at the site. FR is a useful design feature of multi-center RCTs provided it is properly planned for and carefully implemented.
期刊介绍:
BMC Medical Research Methodology is an open access journal publishing original peer-reviewed research articles in methodological approaches to healthcare research. Articles on the methodology of epidemiological research, clinical trials and meta-analysis/systematic review are particularly encouraged, as are empirical studies of the associations between choice of methodology and study outcomes. BMC Medical Research Methodology does not aim to publish articles describing scientific methods or techniques: these should be directed to the BMC journal covering the relevant biomedical subject area.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
