Efficacy and safety of perioperative immunotherapy combinations for resectable non-small cell lung cancer: a systematic review and network meta-analysis.
{"title":"Efficacy and safety of perioperative immunotherapy combinations for resectable non-small cell lung cancer: a systematic review and network meta-analysis.","authors":"Yuelin Han, Xiangtian Xiao, Tingting Qin, Shuxi Yao, Xinyue Liu, Yanqi Feng, Zhou Li, Yiming Li, Shu Xia","doi":"10.1007/s00262-024-03844-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Several trials of perioperative immunotherapy for resectable non-small cell lung cancer (NSCLC) reported positive results. They were designed to adjuvant, neoadjuvant and sandwich (neoadjuvant plus adjuvant) immunotherapy with immune checkpoint inhibitors and chemotherapy (CT). The differences between neoadjuvant and sandwich modalities were unclear.</p><p><strong>Method: </strong>We performed a systematic review and Bayesian network meta-analysis by retrieving relevant literature from PubMed, EMBASE, Cochrane Library, Web of Science, ClinicalTrials.gov, WHO ICTRP and major international conferences.</p><p><strong>Results: </strong>We analyzed 8 studies involving 3429 patients, including 6 neoadjuvant plus adjuvant (Neo-Adj) and 2 neoadjuvant (Neo) trials. Neo-Adj had better event-free survival (EFS) (hazard ratio [HR] = 0.57, 95% confidence interval [CI]: 0.45-0.71) than CT. There existed no difference between Neo-Adj and Neo in EFS (HR = 0.87, 95% CI: 0.53-1.46) and overall survival (OS) (HR = 1.04, 95% CI: 0.38-2.57). Neo might have lower incidence of treatment-related adverse events (TRAEs) (relative risk [RR] = 0.96, 95% CI: 0.87-1.12) than Neo-Adj. Subgroup analysis of PD-L1 ≥ 50% suggested that EFS of Neo-Adj (HR = 0.46, 95% CI: 0.27-0.76) and Neo (HR = 0.24, 95% CI: 0.06-0.89) was better than CT, and Neo-Adj potentially caused shorter EFS than Neo (HR = 1.92, 95% CI: 0.46-7.84).</p><p><strong>Conclusions: </strong>Our results suggest that Neo-Adj and Neo have similar EFS for patients with PD-L1 < 1% or 1-49%. However, patients with PD-L1 ≥ 50% may obtain more EFS benefit from Neo than Neo-Adj. Neo might present a more favorable assessment than Neo-Adj when evaluating OS. Moreover, adding adjuvant immunotherapy may increase toxicity.</p>","PeriodicalId":9595,"journal":{"name":"Cancer Immunology, Immunotherapy","volume":"73 12","pages":"262"},"PeriodicalIF":5.1000,"publicationDate":"2024-10-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11464994/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Immunology, Immunotherapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00262-024-03844-w","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Several trials of perioperative immunotherapy for resectable non-small cell lung cancer (NSCLC) reported positive results. They were designed to adjuvant, neoadjuvant and sandwich (neoadjuvant plus adjuvant) immunotherapy with immune checkpoint inhibitors and chemotherapy (CT). The differences between neoadjuvant and sandwich modalities were unclear.
Method: We performed a systematic review and Bayesian network meta-analysis by retrieving relevant literature from PubMed, EMBASE, Cochrane Library, Web of Science, ClinicalTrials.gov, WHO ICTRP and major international conferences.
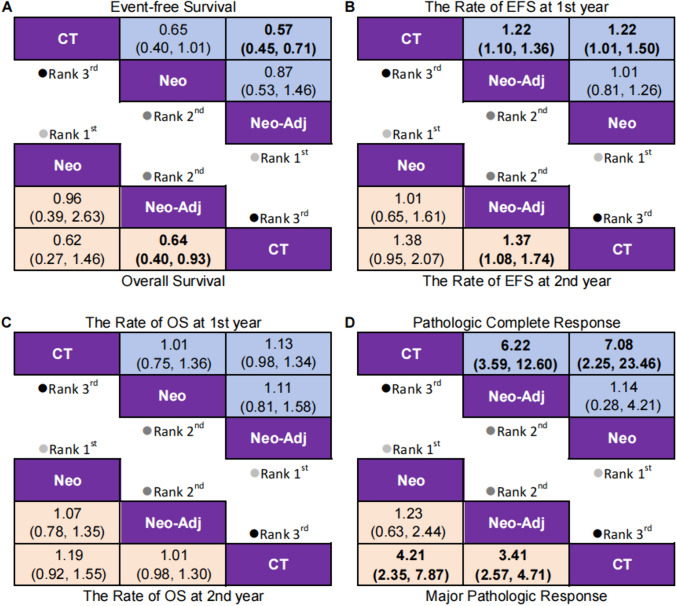
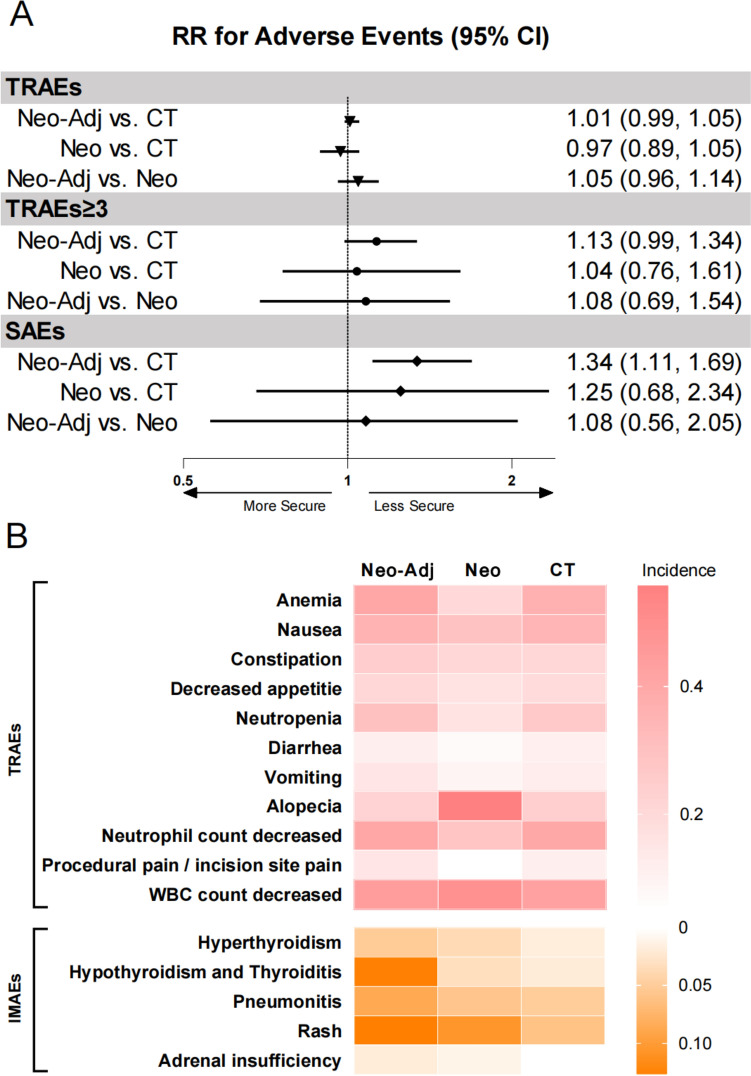
Results: We analyzed 8 studies involving 3429 patients, including 6 neoadjuvant plus adjuvant (Neo-Adj) and 2 neoadjuvant (Neo) trials. Neo-Adj had better event-free survival (EFS) (hazard ratio [HR] = 0.57, 95% confidence interval [CI]: 0.45-0.71) than CT. There existed no difference between Neo-Adj and Neo in EFS (HR = 0.87, 95% CI: 0.53-1.46) and overall survival (OS) (HR = 1.04, 95% CI: 0.38-2.57). Neo might have lower incidence of treatment-related adverse events (TRAEs) (relative risk [RR] = 0.96, 95% CI: 0.87-1.12) than Neo-Adj. Subgroup analysis of PD-L1 ≥ 50% suggested that EFS of Neo-Adj (HR = 0.46, 95% CI: 0.27-0.76) and Neo (HR = 0.24, 95% CI: 0.06-0.89) was better than CT, and Neo-Adj potentially caused shorter EFS than Neo (HR = 1.92, 95% CI: 0.46-7.84).
Conclusions: Our results suggest that Neo-Adj and Neo have similar EFS for patients with PD-L1 < 1% or 1-49%. However, patients with PD-L1 ≥ 50% may obtain more EFS benefit from Neo than Neo-Adj. Neo might present a more favorable assessment than Neo-Adj when evaluating OS. Moreover, adding adjuvant immunotherapy may increase toxicity.
期刊介绍:
Cancer Immunology, Immunotherapy has the basic aim of keeping readers informed of the latest research results in the fields of oncology and immunology. As knowledge expands, the scope of the journal has broadened to include more of the progress being made in the areas of biology concerned with biological response modifiers. This helps keep readers up to date on the latest advances in our understanding of tumor-host interactions.
The journal publishes short editorials including "position papers," general reviews, original articles, and short communications, providing a forum for the most current experimental and clinical advances in tumor immunology.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
