Offir Ukashi, Arad Dotan, Tom Borkovsky, Adi Talan Asher, Tamar Thurm, Ayal Hirsch, Nitsan Maharshak, Eva Niv, Moshe Leshno, Rami Eliakim, Shomron Ben-Horin, Uri Kopylov, Liat Deutsch
{"title":"Pro-motility Preparation Protocol May Reduce the Rates of Failed Patency Capsule Among Patients with Crohn's Disease in Clinical Remission.","authors":"Offir Ukashi, Arad Dotan, Tom Borkovsky, Adi Talan Asher, Tamar Thurm, Ayal Hirsch, Nitsan Maharshak, Eva Niv, Moshe Leshno, Rami Eliakim, Shomron Ben-Horin, Uri Kopylov, Liat Deutsch","doi":"10.1007/s10620-024-08670-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patency capsule (PC) ingestion is commonly used to minimize capsule retention in high-risk patients with Crohn's disease (CD). However, false-positive rates remain high, precluding the use of video capsule endoscopy (VCE). We aimed to compare the efficacy of two preparation protocols in reducing failed PC rates in patients with CD.</p><p><strong>Methods: </strong>This bi-center retrospective case-control study included adult patients with small-bowel CD in clinical remission who underwent PC ingestion. The pro-motility group followed a low-residue diet, then a clear fluid diet, and took bisacodyl after ingestion, while the control group followed only a clear fluid diet. The primary outcome was failed PC, defined as the absence of PC excretion or presence on abdominal X-ray at 30 h post-ingestion. Multivariable logistic regression was used to identify predictors of failed PC.</p><p><strong>Results: </strong>Among 273 patients (83 in the pro-motility group, 190 controls), the pro-motility group was older (median 36 [27-48] vs. 31 [24-43], p = 0.012) and had a lower rate of B2/3 disease phenotype (32.5 vs. 53.1%, p = 0.002) compared to controls. The pro-motility group also had a lower failed PC rate (12.0 vs. 24.7%, p = 0.023). Longer disease duration (adjusted odds ratio (AOR) 1.053, 95% confidence interval (CI) 1.016-1.091, p = 0.005) increased the odds of failed PC, while the pro-motility protocol was protective (AOR 0.438, 95% CI 0.200-0.956, p = 0.038), outweighing the influence of B2/3 disease phenotype (AOR 1.743, 95% CI 0.912-3.332, p = 0.093).</p><p><strong>Conclusions: </strong>The pro-motility preparation protocol could substantially improve the success rates of the small-bowel patency test in patients with CD undergoing PC ingestion, potentially reducing the risk of capsule retention and associated complications.</p>","PeriodicalId":11378,"journal":{"name":"Digestive Diseases and Sciences","volume":" ","pages":"4178-4186"},"PeriodicalIF":2.5000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11568050/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Diseases and Sciences","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10620-024-08670-9","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/9 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patency capsule (PC) ingestion is commonly used to minimize capsule retention in high-risk patients with Crohn's disease (CD). However, false-positive rates remain high, precluding the use of video capsule endoscopy (VCE). We aimed to compare the efficacy of two preparation protocols in reducing failed PC rates in patients with CD.
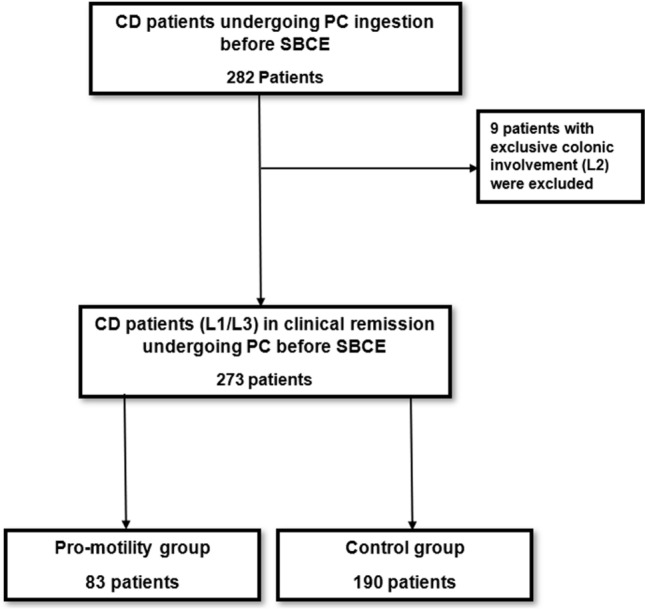
Methods: This bi-center retrospective case-control study included adult patients with small-bowel CD in clinical remission who underwent PC ingestion. The pro-motility group followed a low-residue diet, then a clear fluid diet, and took bisacodyl after ingestion, while the control group followed only a clear fluid diet. The primary outcome was failed PC, defined as the absence of PC excretion or presence on abdominal X-ray at 30 h post-ingestion. Multivariable logistic regression was used to identify predictors of failed PC.
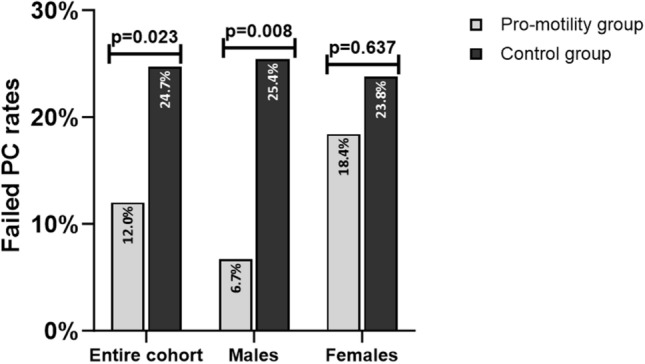
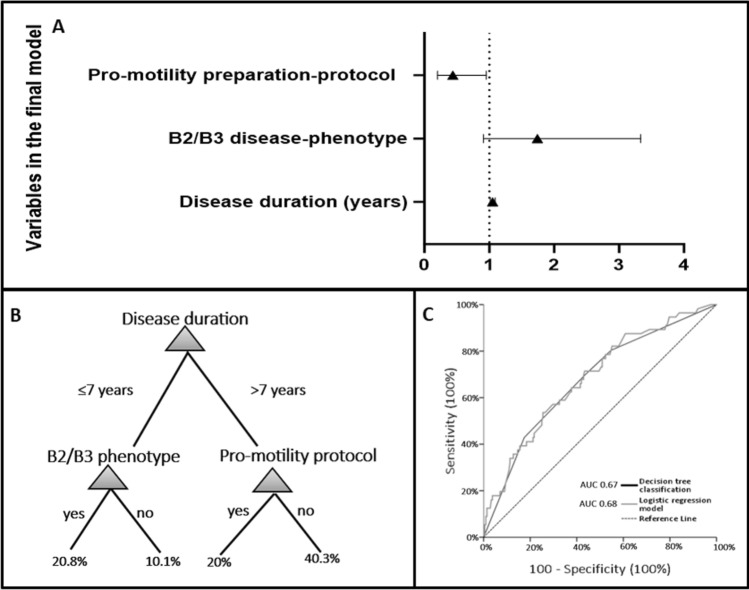
Results: Among 273 patients (83 in the pro-motility group, 190 controls), the pro-motility group was older (median 36 [27-48] vs. 31 [24-43], p = 0.012) and had a lower rate of B2/3 disease phenotype (32.5 vs. 53.1%, p = 0.002) compared to controls. The pro-motility group also had a lower failed PC rate (12.0 vs. 24.7%, p = 0.023). Longer disease duration (adjusted odds ratio (AOR) 1.053, 95% confidence interval (CI) 1.016-1.091, p = 0.005) increased the odds of failed PC, while the pro-motility protocol was protective (AOR 0.438, 95% CI 0.200-0.956, p = 0.038), outweighing the influence of B2/3 disease phenotype (AOR 1.743, 95% CI 0.912-3.332, p = 0.093).
Conclusions: The pro-motility preparation protocol could substantially improve the success rates of the small-bowel patency test in patients with CD undergoing PC ingestion, potentially reducing the risk of capsule retention and associated complications.
背景:在克罗恩病(CD)高危患者中,摄入通畅胶囊(PC)通常用于减少胶囊滞留。然而,假阳性率仍然很高,导致无法使用视频胶囊内镜(VCE)。我们旨在比较两种准备方案在降低 CD 患者 PC 检查失败率方面的效果:这项双中心回顾性病例对照研究纳入了临床缓解期的小肠 CD 成年患者,他们都接受了 PC 摄取。促进肠蠕动组先摄入低渣饮食,然后摄入清流饮食,并在摄入后服用比沙可啶,而对照组仅摄入清流饮食。主要结果是 PC 失败,即进食后 30 小时无 PC 排泄或腹部 X 光片上出现 PC。多变量逻辑回归用于确定 PC 失败的预测因素:在 273 名患者中(83 名为顺应性组,190 名为对照组),与对照组相比,顺应性组患者年龄较大(中位数为 36 [27-48] 对 31 [24-43],p = 0.012),B2/3 疾病表型比例较低(32.5 对 53.1%,p = 0.002)。促流动组的 PC 失败率也较低(12.0% 对 24.7%,p = 0.023)。病程较长(调整后比值比(AOR)1.053,95% 置信区间(CI)1.016-1.091,p = 0.005)会增加PC失败的几率,而支持运动方案具有保护作用(AOR 0.438,95% CI 0.200-0.956,p = 0.038),超过了B2/3疾病表型(AOR 1.743,95% CI 0.912-3.332,p = 0.093)的影响:结论:促进肠蠕动的准备方案可大大提高接受PC摄取的CD患者小肠通畅试验的成功率,从而降低胶囊滞留和相关并发症的风险。
期刊介绍:
Digestive Diseases and Sciences publishes high-quality, peer-reviewed, original papers addressing aspects of basic/translational and clinical research in gastroenterology, hepatology, and related fields. This well-illustrated journal features comprehensive coverage of basic pathophysiology, new technological advances, and clinical breakthroughs; insights from prominent academicians and practitioners concerning new scientific developments and practical medical issues; and discussions focusing on the latest changes in local and worldwide social, economic, and governmental policies that affect the delivery of care within the disciplines of gastroenterology and hepatology.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
