Zhixing Song, Jessica McMullin, Forest Huls, Richard Rosenthal, Sravani Bantu, Christopher Wu, Herbert Chen, Brenessa Lindeman
{"title":"Primary Hyperparathyroidism With Undetectable Intact Parathyroid Hormone.","authors":"Zhixing Song, Jessica McMullin, Forest Huls, Richard Rosenthal, Sravani Bantu, Christopher Wu, Herbert Chen, Brenessa Lindeman","doi":"10.1177/11795514241290125","DOIUrl":null,"url":null,"abstract":"<p><p>Hypercalcemia can result from either hyperparathyroidism or non-parathyroid conditions. When hypercalcemia is accompanied by undetectable parathyroid hormone (PTH) levels, hyperparathyroidism is rarely considered the diagnosis. Herein, we report the case of a 65-year-old Caucasian woman referred to our hospital for further evaluation of hypercalcemia. Her symptoms included fatigue and brain fog, with undetectable PTH levels. A comprehensive workup, including a series of laboratory and imaging tests, excluded common non-parathyroid causes such as malignancy and familial hypocalciuric hypercalcemia. Ultrasound identified a likely enlarged parathyroid gland, which was further confirmed by a sestamibi scan. After 2 weeks of cinacalcet treatment, the patient's calcium levels decreased, indicating the parathyroid gland as the likely source of hypercalcemia. Parathyroidectomy was subsequently performed, revealing a 1927 mg adenoma. Postoperatively, the patient's calcium levels normalized, PTH levels became detectable within the normal range, and her symptoms resolved, with a marked improvement in energy. This case demonstrates that primary hyperparathyroidism can present with hypercalcemia and undetectable PTH. A genetic mutation in the PTH gene within the adenoma may explain the undetectable PTH levels preoperatively.</p>","PeriodicalId":44715,"journal":{"name":"Clinical Medicine Insights-Endocrinology and Diabetes","volume":"17 ","pages":"11795514241290125"},"PeriodicalIF":3.0000,"publicationDate":"2024-10-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11459549/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Endocrinology and Diabetes","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795514241290125","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
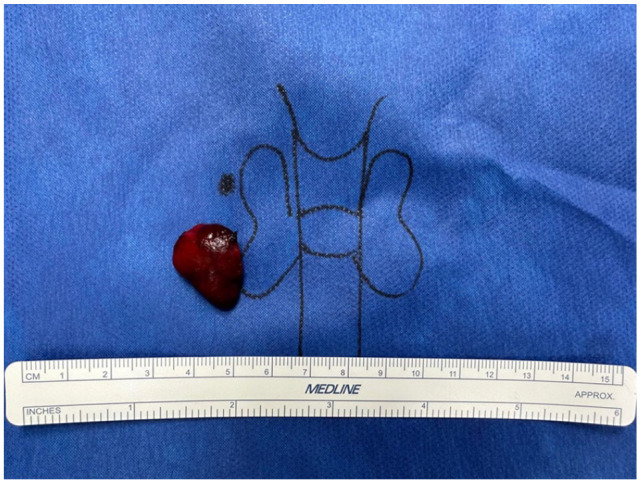
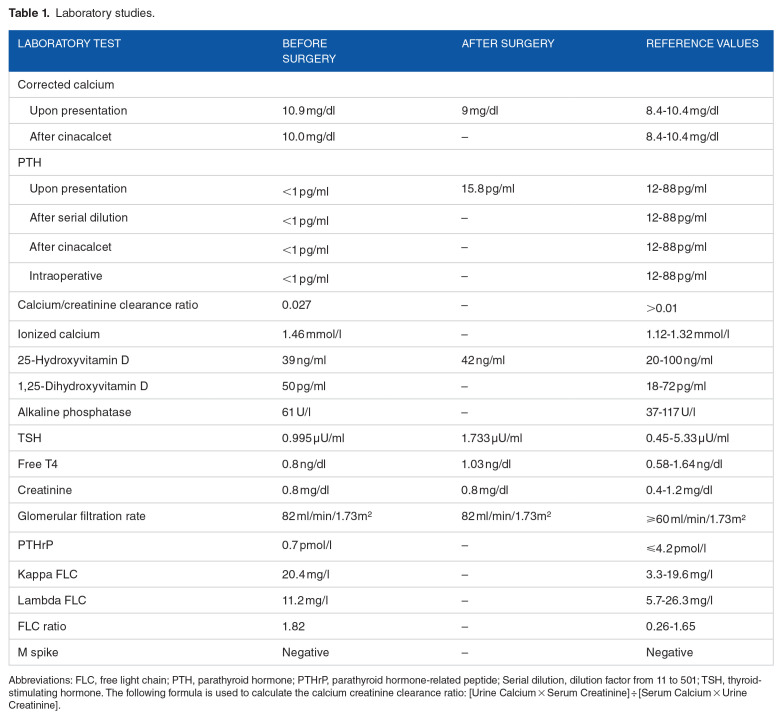
Hypercalcemia can result from either hyperparathyroidism or non-parathyroid conditions. When hypercalcemia is accompanied by undetectable parathyroid hormone (PTH) levels, hyperparathyroidism is rarely considered the diagnosis. Herein, we report the case of a 65-year-old Caucasian woman referred to our hospital for further evaluation of hypercalcemia. Her symptoms included fatigue and brain fog, with undetectable PTH levels. A comprehensive workup, including a series of laboratory and imaging tests, excluded common non-parathyroid causes such as malignancy and familial hypocalciuric hypercalcemia. Ultrasound identified a likely enlarged parathyroid gland, which was further confirmed by a sestamibi scan. After 2 weeks of cinacalcet treatment, the patient's calcium levels decreased, indicating the parathyroid gland as the likely source of hypercalcemia. Parathyroidectomy was subsequently performed, revealing a 1927 mg adenoma. Postoperatively, the patient's calcium levels normalized, PTH levels became detectable within the normal range, and her symptoms resolved, with a marked improvement in energy. This case demonstrates that primary hyperparathyroidism can present with hypercalcemia and undetectable PTH. A genetic mutation in the PTH gene within the adenoma may explain the undetectable PTH levels preoperatively.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
