Eric P Borrelli, Peter Saad, Nathan E Barnes, Doina Dumitru, Julia D Lucaci
{"title":"Improving Adherence and Reducing Health Care Costs Through Blister-Packaging: An Economic Model for a Commercially Insured Health Plan.","authors":"Eric P Borrelli, Peter Saad, Nathan E Barnes, Doina Dumitru, Julia D Lucaci","doi":"10.2147/CEOR.S480890","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To model the potential clinical and economic impact of blister-packaging medications for chronic conditions on medication adherence and healthcare costs in a commercially insured population.</p><p><strong>Methods: </strong>A health economic model was developed to evaluate the potential impact of blister-packaging chronic medications for a commercially insured population. The chronic medication classes assessed were renin-angiotensin-system (RAS) antagonists, statins, non-insulin oral antidiabetics, and direct oral anticoagulants (DOACs). The model was designed to reflect the perspective of a hypothetical commercially insured health plan with 100,000 members, over a one-year time horizon. Literature-based or best available epidemiologic references were used to inform the number of patients utilizing each medication class, the impact of blister-packaging on the number of patients who become adherent, as well as the impact of medication adherence in a commercially insured population on healthcare costs for each medication class assessed. Impact on costs was measured in total net healthcare costs, as well as being stratified by medical costs and medication costs.</p><p><strong>Results: </strong>Following the blister-packaging intervention, there were an additional 591 patients adherent to RAS antagonists, 1196 patients adherent to statins, 169 patients adherent to oral antidiabetics, and 25 patients adherent to DOACs. While pharmacy costs increased, these costs were more than offset by the reduction in medical costs. Overall, the increase in patients adherent to therapy due to blister-packaging led to a reduction in total healthcare costs of $879,312 for RAS antagonists (-$0.73 per-member per-month (PMPM)), $343,322 for statins (-$0.29 PMPM), $78,917 for oral antidiabetics (-$0.07 PMPM), and $120,793 for DOACs (-$0.10 PMPM).</p><p><strong>Conclusion: </strong>Blister-packaging chronic medications in a commercially insured population has the potential to reduce healthcare costs. Future research is needed to confirm these findings in real-world settings and to fully understand the clinical and economic implications of blister-packaging chronic medications.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"16 ","pages":"733-745"},"PeriodicalIF":2.2000,"publicationDate":"2024-10-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11457784/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S480890","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To model the potential clinical and economic impact of blister-packaging medications for chronic conditions on medication adherence and healthcare costs in a commercially insured population.
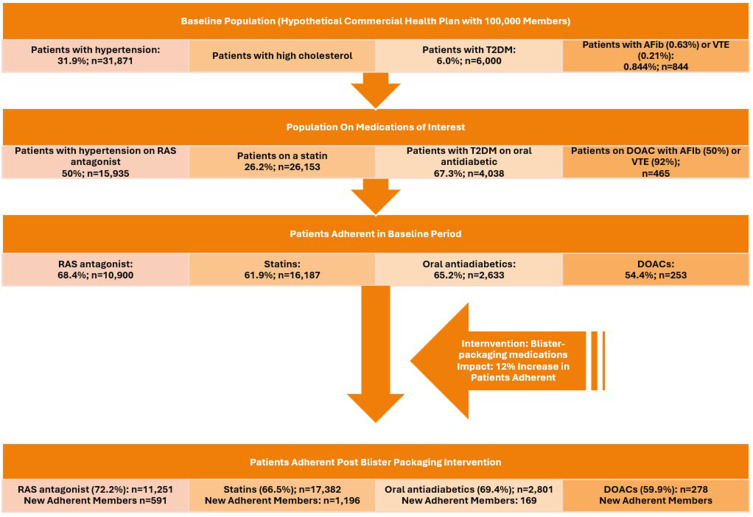
Methods: A health economic model was developed to evaluate the potential impact of blister-packaging chronic medications for a commercially insured population. The chronic medication classes assessed were renin-angiotensin-system (RAS) antagonists, statins, non-insulin oral antidiabetics, and direct oral anticoagulants (DOACs). The model was designed to reflect the perspective of a hypothetical commercially insured health plan with 100,000 members, over a one-year time horizon. Literature-based or best available epidemiologic references were used to inform the number of patients utilizing each medication class, the impact of blister-packaging on the number of patients who become adherent, as well as the impact of medication adherence in a commercially insured population on healthcare costs for each medication class assessed. Impact on costs was measured in total net healthcare costs, as well as being stratified by medical costs and medication costs.
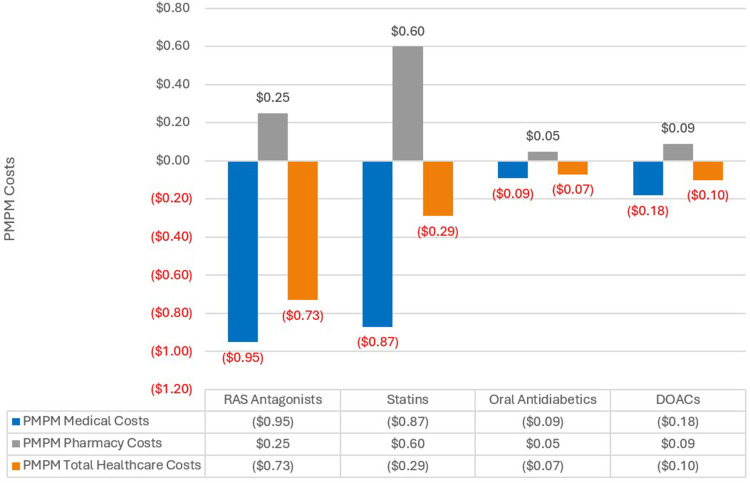
Results: Following the blister-packaging intervention, there were an additional 591 patients adherent to RAS antagonists, 1196 patients adherent to statins, 169 patients adherent to oral antidiabetics, and 25 patients adherent to DOACs. While pharmacy costs increased, these costs were more than offset by the reduction in medical costs. Overall, the increase in patients adherent to therapy due to blister-packaging led to a reduction in total healthcare costs of $879,312 for RAS antagonists (-$0.73 per-member per-month (PMPM)), $343,322 for statins (-$0.29 PMPM), $78,917 for oral antidiabetics (-$0.07 PMPM), and $120,793 for DOACs (-$0.10 PMPM).
Conclusion: Blister-packaging chronic medications in a commercially insured population has the potential to reduce healthcare costs. Future research is needed to confirm these findings in real-world settings and to fully understand the clinical and economic implications of blister-packaging chronic medications.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
