Prediction of non-resectability in tubo-ovarian cancer patients using Peritoneal Cancer Index – A prospective multicentric study using imaging (ISAAC study)
Patrícia Pinto , Francesca Moro , Juan Luis Alcázar , Sarah Alessi , Giacomo Avesani , Klára Benesova , Andrea Burgetova , Giuseppina Calareso , Valentina Chiappa , David Cibula , Anna Fagotti , Dorella Franchi , Filip Frühauf , Jiri Jarkovsky , Roman Kocian , Lukas Lambert , Martin Masek , Camilla Panico , Paola Pricolo , Giovanni Scambia , Daniela Fischerová
{"title":"Prediction of non-resectability in tubo-ovarian cancer patients using Peritoneal Cancer Index – A prospective multicentric study using imaging (ISAAC study)","authors":"Patrícia Pinto , Francesca Moro , Juan Luis Alcázar , Sarah Alessi , Giacomo Avesani , Klára Benesova , Andrea Burgetova , Giuseppina Calareso , Valentina Chiappa , David Cibula , Anna Fagotti , Dorella Franchi , Filip Frühauf , Jiri Jarkovsky , Roman Kocian , Lukas Lambert , Martin Masek , Camilla Panico , Paola Pricolo , Giovanni Scambia , Daniela Fischerová","doi":"10.1016/j.ygyno.2024.10.003","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>The aim was to evaluate the performance of the Peritoneal Cancer Index (PCI) using imaging (ultrasound, contrast-enhanced computed tomography (CT), and whole-body diffusion-weighted magnetic resonance imaging (WB-DWI/MRI) in assessing peritoneal carcinomatosis and predicting non-resectability in tubo-ovarian carcinoma patients.</div></div><div><h3>Methods</h3><div>This was a prospective multicenter observational study. We considered all patients with suspected primary ovarian/tubal/peritoneal cancer who underwent preoperative ultrasound, CT, and WB-DWI/MRI (if available). The optimal cut off value for assessing the performance of the methods in predicting non-resectability was identified at the point at which the sensitivity and specificity were most similar. The reference standard to predict non-resectability was surgical outcome in terms of residual disease >1 cm or surgery not feasible. Agreement between imaging methods and surgical exploration in assessing sites included in the PCI score was evaluated using the Intraclass Correlation Coefficient (ICC).</div></div><div><h3>Results</h3><div>242 patients were included from January 2020 until November 2022. The optimal PCI cut-off for predicting non-resectability for surgical exploration was >12, which achieved the best AUC of 0.87, followed by ultrasound with a cut-off of >10 and AUC of 0.81, WB-DWI/MRI with a cut-off of >12 and AUC of 0.81, and CT with a cut-off of >11 and AUC of 0.74. Using ICC, ultrasound had very high agreement (0.94) with surgical PCI, while CT and WB-DWI/MRI had high agreement (0.86 and 0.87, respectively).</div></div><div><h3>Conclusion</h3><div>Ultrasound performed by an expert operator had the best agreement with surgical findings compared to WB-DWI/MRI and CT in assessing radiological PCI. In predicting non-resectability, ultrasound was non-inferior to CT, while its non-inferiority to WB-DWI/MRI was not demonstrated.</div></div>","PeriodicalId":12853,"journal":{"name":"Gynecologic oncology","volume":"191 ","pages":"Pages 132-142"},"PeriodicalIF":4.5000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gynecologic oncology","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0090825824011533","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/10 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
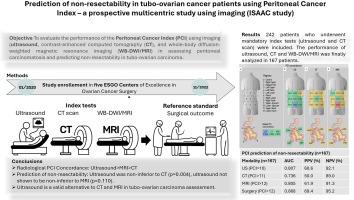
The aim was to evaluate the performance of the Peritoneal Cancer Index (PCI) using imaging (ultrasound, contrast-enhanced computed tomography (CT), and whole-body diffusion-weighted magnetic resonance imaging (WB-DWI/MRI) in assessing peritoneal carcinomatosis and predicting non-resectability in tubo-ovarian carcinoma patients.
Methods
This was a prospective multicenter observational study. We considered all patients with suspected primary ovarian/tubal/peritoneal cancer who underwent preoperative ultrasound, CT, and WB-DWI/MRI (if available). The optimal cut off value for assessing the performance of the methods in predicting non-resectability was identified at the point at which the sensitivity and specificity were most similar. The reference standard to predict non-resectability was surgical outcome in terms of residual disease >1 cm or surgery not feasible. Agreement between imaging methods and surgical exploration in assessing sites included in the PCI score was evaluated using the Intraclass Correlation Coefficient (ICC).
Results
242 patients were included from January 2020 until November 2022. The optimal PCI cut-off for predicting non-resectability for surgical exploration was >12, which achieved the best AUC of 0.87, followed by ultrasound with a cut-off of >10 and AUC of 0.81, WB-DWI/MRI with a cut-off of >12 and AUC of 0.81, and CT with a cut-off of >11 and AUC of 0.74. Using ICC, ultrasound had very high agreement (0.94) with surgical PCI, while CT and WB-DWI/MRI had high agreement (0.86 and 0.87, respectively).
Conclusion
Ultrasound performed by an expert operator had the best agreement with surgical findings compared to WB-DWI/MRI and CT in assessing radiological PCI. In predicting non-resectability, ultrasound was non-inferior to CT, while its non-inferiority to WB-DWI/MRI was not demonstrated.
期刊介绍:
Gynecologic Oncology, an international journal, is devoted to the publication of clinical and investigative articles that concern tumors of the female reproductive tract. Investigations relating to the etiology, diagnosis, and treatment of female cancers, as well as research from any of the disciplines related to this field of interest, are published.
Research Areas Include:
• Cell and molecular biology
• Chemotherapy
• Cytology
• Endocrinology
• Epidemiology
• Genetics
• Gynecologic surgery
• Immunology
• Pathology
• Radiotherapy




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
