Ming-Jer Hsieh , Jih-Kai Yeh , Yu-Chang Huang , Ming-Yun Ho , Dong-Yi Chen , Cheng-Hung Lee , Chao-Yung Wang , Shang-Hung Chang , Chun-Chi Chen , I-Chang Hsieh
{"title":"Cardiac power output associated with hospitalization and mortality in coronary artery disease patients at stage B heart failure","authors":"Ming-Jer Hsieh , Jih-Kai Yeh , Yu-Chang Huang , Ming-Yun Ho , Dong-Yi Chen , Cheng-Hung Lee , Chao-Yung Wang , Shang-Hung Chang , Chun-Chi Chen , I-Chang Hsieh","doi":"10.1016/j.ijcha.2024.101521","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>Cardiac power output (CPO) predicts outcomes in advanced heart failure (HF) and cardiogenic shock, but its role in early HF stages is unclear. This study assessed the prognostic value of CPO in coronary artery disease patients with asymptomatic left ventricular systolic dysfunction (ALVSD) at stage B HF.</div></div><div><h3>Methods</h3><div>We conducted a retrospective analysis of coronary artery disease patients who underwent coronary and pulmonary artery catheterization between 2006 and 2016. Stage B HF with ALVSD was defined as left ventricular ejection fraction < 50 %, without HF symptoms, signs, or prior HF hospitalization. CPO was derived from invasive hemodynamic parameters. Endpoints included HF hospitalization, cardiovascular mortality, and all-cause mortality over a 5-year follow-up.</div></div><div><h3>Results</h3><div>A total of 783 coronary artery disease patients with ALVSD at stage B HF were enrolled. Incidence rates (per 1000 person-years) were 13.9 for HF hospitalization, 14.5 for cardiovascular mortality, and 23.7 for all-cause mortality.Multivariate analysis adjusting for covariates demonstrated that CPO was independent associated with all endpoints. Patients with a low CPO (<0.97 Watts) were at significantly higher risk for HF hospitalization (adjusted hazard ratio [HR]: 4.04; 95 % CI: 1.53 – 10.6; p = 0.005), cardiovascular mortality (adjusted HR: 2.73; 95 % CI: 1.19 – 6.27; p = 0.018), and all-cause mortality (adjusted HR: 1.86; 95 % CI: 1.05 – 3.30; p = 0.035) compared to those with higher CPO, regardless of subgroup classification.</div></div><div><h3>Conclusion</h3><div>Resting CPO in patients with ALVSD is significantly associated with adverse events, including HF hospitalization and mortality, highlighting its value in early-stage HF management.</div></div>","PeriodicalId":38026,"journal":{"name":"IJC Heart and Vasculature","volume":"55 ","pages":"Article 101521"},"PeriodicalIF":2.5000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"IJC Heart and Vasculature","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2352906724001878","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/4 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
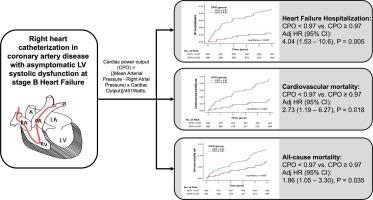
Cardiac power output (CPO) predicts outcomes in advanced heart failure (HF) and cardiogenic shock, but its role in early HF stages is unclear. This study assessed the prognostic value of CPO in coronary artery disease patients with asymptomatic left ventricular systolic dysfunction (ALVSD) at stage B HF.
Methods
We conducted a retrospective analysis of coronary artery disease patients who underwent coronary and pulmonary artery catheterization between 2006 and 2016. Stage B HF with ALVSD was defined as left ventricular ejection fraction < 50 %, without HF symptoms, signs, or prior HF hospitalization. CPO was derived from invasive hemodynamic parameters. Endpoints included HF hospitalization, cardiovascular mortality, and all-cause mortality over a 5-year follow-up.
Results
A total of 783 coronary artery disease patients with ALVSD at stage B HF were enrolled. Incidence rates (per 1000 person-years) were 13.9 for HF hospitalization, 14.5 for cardiovascular mortality, and 23.7 for all-cause mortality.Multivariate analysis adjusting for covariates demonstrated that CPO was independent associated with all endpoints. Patients with a low CPO (<0.97 Watts) were at significantly higher risk for HF hospitalization (adjusted hazard ratio [HR]: 4.04; 95 % CI: 1.53 – 10.6; p = 0.005), cardiovascular mortality (adjusted HR: 2.73; 95 % CI: 1.19 – 6.27; p = 0.018), and all-cause mortality (adjusted HR: 1.86; 95 % CI: 1.05 – 3.30; p = 0.035) compared to those with higher CPO, regardless of subgroup classification.
Conclusion
Resting CPO in patients with ALVSD is significantly associated with adverse events, including HF hospitalization and mortality, highlighting its value in early-stage HF management.
期刊介绍:
IJC Heart & Vasculature is an online-only, open-access journal dedicated to publishing original articles and reviews (also Editorials and Letters to the Editor) which report on structural and functional cardiovascular pathology, with an emphasis on imaging and disease pathophysiology. Articles must be authentic, educational, clinically relevant, and original in their content and scientific approach. IJC Heart & Vasculature requires the highest standards of scientific integrity in order to promote reliable, reproducible and verifiable research findings. All authors are advised to consult the Principles of Ethical Publishing in the International Journal of Cardiology before submitting a manuscript. Submission of a manuscript to this journal gives the publisher the right to publish that paper if it is accepted. Manuscripts may be edited to improve clarity and expression.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
