Yu-Xuan Jiang MD, Chun-Gu Cheng MD, Yen-Yue Lin MD
{"title":"Man with left-sided flank pain","authors":"Yu-Xuan Jiang MD, Chun-Gu Cheng MD, Yen-Yue Lin MD","doi":"10.1002/emp2.13326","DOIUrl":null,"url":null,"abstract":"<p>A 35-year-old man with alcohol abuse presented to the emergency department with a 7-day history of cough and left-sided flank pain. His temperature, pulse rate, and blood pressure were 38.1°C, 104 beats/min, and 134/92 mmHg, respectively. Based on physical examination, his breath sounds were smooth without crackles; whereas, the left flank region was tender to palpation. His white blood cell count, platelet count, and C-reactive protein were 17,740/µL, 1101 × 10<sup>3</sup> mm, and 18.5 mg/dL, respectively. An emergency physician performed ultrasonography revealing heterogeneous echoic lesions in the spleen (Figure 1), and the diagnosis was confirmed by computed tomography (Figure 2).</p><p>The patient received antibiotic treatment (moxifloxacin), laparoscopic splenectomy, and pus drainage by a surgeon (Figure 3). The tissue culture of the spleen grew <i>Streptococcus constellatus</i>.</p><p>Splenic abscess is an uncommon life-threatening disease, with incidence ranging from 0.14% to 0.7%. However, the patients are at high risk of mortality if appropriate treatment is not administered. The clinical presentation of fever, left upper quadrant tenderness, and leukocytosis is not usually present. It potentially causes misdiagnosis in patients presenting with nonspecific symptoms, such as cough, abdominal pain, back pain, and malaise.<span><sup>1</sup></span> Splenectomy is the gold standard treatment for splenic abscess. Percutaneous drainage can be an alternative therapy in patients with high surgical risk.<span><sup>2</sup></span></p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":73967,"journal":{"name":"Journal of the American College of Emergency Physicians open","volume":"5 5","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-10-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/emp2.13326","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Emergency Physicians open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13326","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
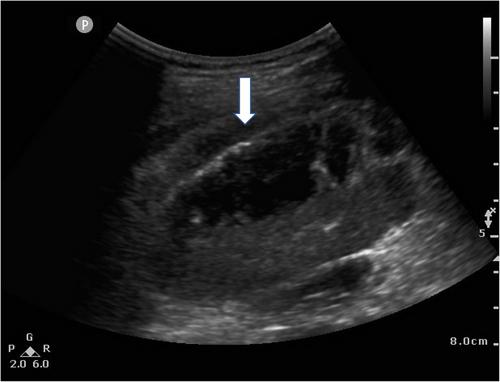
A 35-year-old man with alcohol abuse presented to the emergency department with a 7-day history of cough and left-sided flank pain. His temperature, pulse rate, and blood pressure were 38.1°C, 104 beats/min, and 134/92 mmHg, respectively. Based on physical examination, his breath sounds were smooth without crackles; whereas, the left flank region was tender to palpation. His white blood cell count, platelet count, and C-reactive protein were 17,740/µL, 1101 × 103 mm, and 18.5 mg/dL, respectively. An emergency physician performed ultrasonography revealing heterogeneous echoic lesions in the spleen (Figure 1), and the diagnosis was confirmed by computed tomography (Figure 2).
The patient received antibiotic treatment (moxifloxacin), laparoscopic splenectomy, and pus drainage by a surgeon (Figure 3). The tissue culture of the spleen grew Streptococcus constellatus.
Splenic abscess is an uncommon life-threatening disease, with incidence ranging from 0.14% to 0.7%. However, the patients are at high risk of mortality if appropriate treatment is not administered. The clinical presentation of fever, left upper quadrant tenderness, and leukocytosis is not usually present. It potentially causes misdiagnosis in patients presenting with nonspecific symptoms, such as cough, abdominal pain, back pain, and malaise.1 Splenectomy is the gold standard treatment for splenic abscess. Percutaneous drainage can be an alternative therapy in patients with high surgical risk.2


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
