Comparison of Hounsfield Unit, Vertebral Bone Quality, and Dual-Energy X-Ray Absorptiometry T-Score for Predicting Cage Subsidence After Posterior Lumbar Interbody Fusion.
{"title":"Comparison of Hounsfield Unit, Vertebral Bone Quality, and Dual-Energy X-Ray Absorptiometry T-Score for Predicting Cage Subsidence After Posterior Lumbar Interbody Fusion.","authors":"Yunsheng Wang, Jiali Zhang, Tong Tong, Dechao Miao, Feng Wang, Linfeng Wang","doi":"10.1177/21925682241293038","DOIUrl":null,"url":null,"abstract":"<p><p>Study designRetrospective cohort study.ObjectivesTo compare Hounsfield unit (HU), vertebral bone quality (VBQ), and dual-energy X-ray absorptiometry (DEXA) T-score in predicting cage subsidence (CS) after posterior lumbar interbody fusion.MethodsWe retrospectively reviewed patients undergoing PLIF and measured L4 HU and VBQ. Baseline characteristics between CS and non-CS groups were compared. Multiple logistic regression analysis was used to identify risk factors for CS. Receiver operating characteristic (ROC) curves were used to explore the predictive value of variables for CS. Subgroup analysis was conducted for patients with available DEXA results.ResultsEighty-four patients were analyzed. The subsidence group was older, with lower L4 HU (92.6 (35.4) vs 130.8 (47.8), <i>P</i> < 0.001) and higher VBQ (3.30 (0.64) vs 2.99 (0.63), <i>P</i> = 0.041) compared to the non-CS group. Low L4 HU (OR 0.979, <i>P</i> = 0.022) was an independent risk factor for subsidence, while VBQ was not. ROC analysis indicated that L4 HU (AUC = 0.733, <i>P</i> < 0.001) exhibited superior predictive performance compared to VBQ (AUC = 0.643, <i>P</i> = 0.032). Subgroup analysis in patients with DEXA showed that the femoral neck T-score (AUC = 0.67, <i>P</i> = 0.037) could differentiate CS, with L4 HU exhibiting the highest predictive ability (AUC = 0.778, <i>P</i> < 0.001), both outperforming VBQ (AUC = 0.645, <i>P</i> = 0.075).ConclusionsAmong the three BMD parameters, only low L4 HU could be an independent risk factor for CS. Preoperative HU is mandatory in patients at risk for osteoporosis when undergoing spine surgery.</p>","PeriodicalId":12680,"journal":{"name":"Global Spine Journal","volume":" ","pages":"2226-2235"},"PeriodicalIF":3.0000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11559888/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Spine Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/21925682241293038","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/14 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
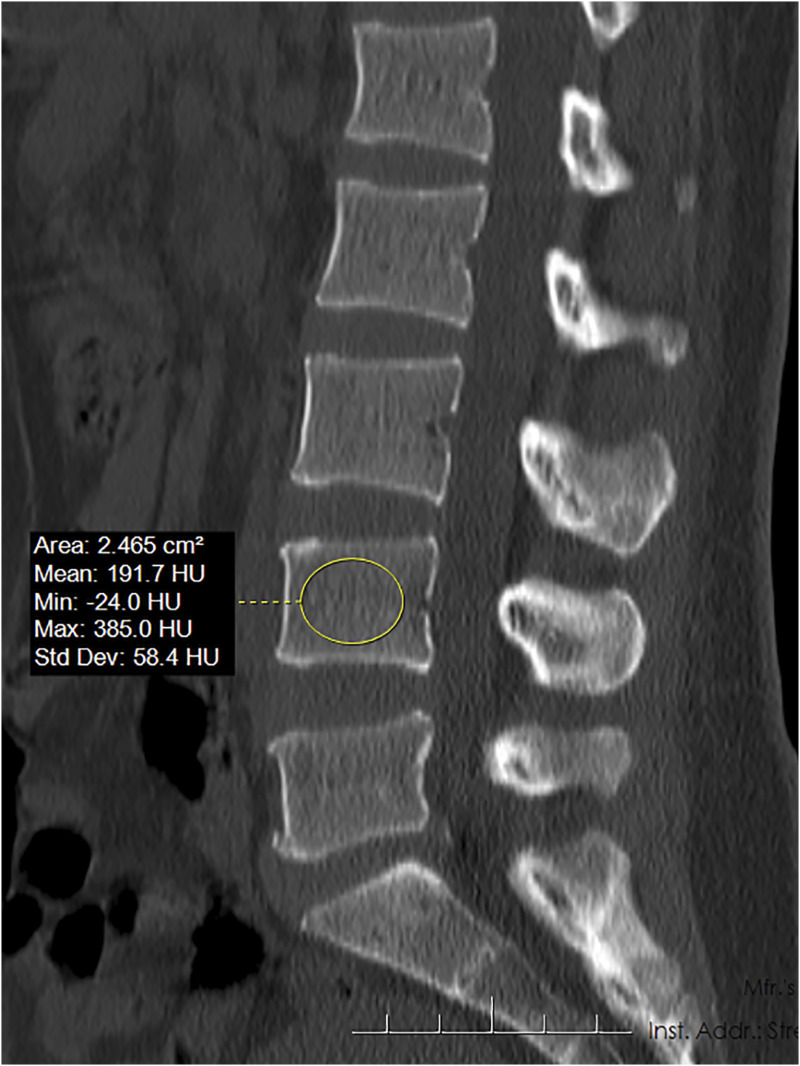
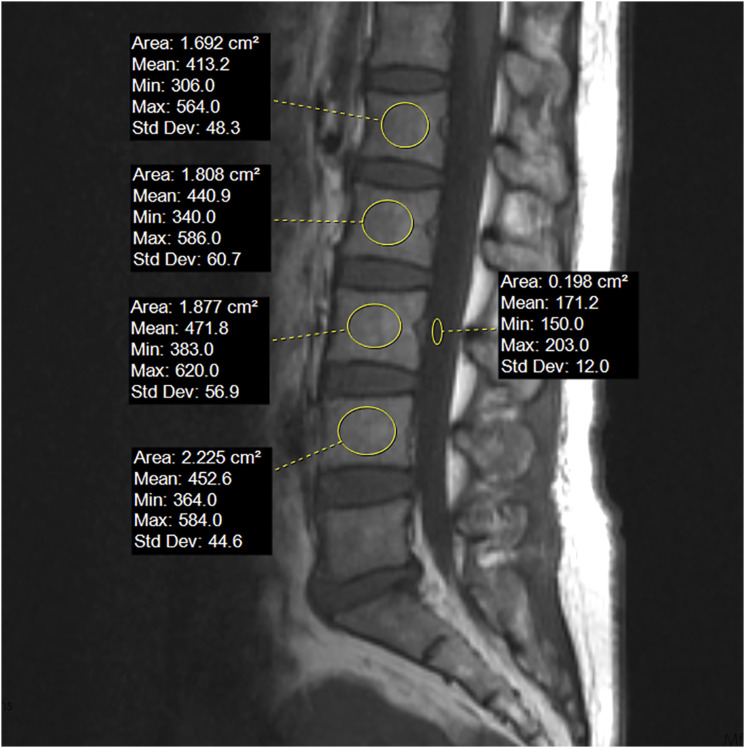
Study designRetrospective cohort study.ObjectivesTo compare Hounsfield unit (HU), vertebral bone quality (VBQ), and dual-energy X-ray absorptiometry (DEXA) T-score in predicting cage subsidence (CS) after posterior lumbar interbody fusion.MethodsWe retrospectively reviewed patients undergoing PLIF and measured L4 HU and VBQ. Baseline characteristics between CS and non-CS groups were compared. Multiple logistic regression analysis was used to identify risk factors for CS. Receiver operating characteristic (ROC) curves were used to explore the predictive value of variables for CS. Subgroup analysis was conducted for patients with available DEXA results.ResultsEighty-four patients were analyzed. The subsidence group was older, with lower L4 HU (92.6 (35.4) vs 130.8 (47.8), P < 0.001) and higher VBQ (3.30 (0.64) vs 2.99 (0.63), P = 0.041) compared to the non-CS group. Low L4 HU (OR 0.979, P = 0.022) was an independent risk factor for subsidence, while VBQ was not. ROC analysis indicated that L4 HU (AUC = 0.733, P < 0.001) exhibited superior predictive performance compared to VBQ (AUC = 0.643, P = 0.032). Subgroup analysis in patients with DEXA showed that the femoral neck T-score (AUC = 0.67, P = 0.037) could differentiate CS, with L4 HU exhibiting the highest predictive ability (AUC = 0.778, P < 0.001), both outperforming VBQ (AUC = 0.645, P = 0.075).ConclusionsAmong the three BMD parameters, only low L4 HU could be an independent risk factor for CS. Preoperative HU is mandatory in patients at risk for osteoporosis when undergoing spine surgery.
期刊介绍:
Global Spine Journal (GSJ) is the official scientific publication of AOSpine. A peer-reviewed, open access journal, devoted to the study and treatment of spinal disorders, including diagnosis, operative and non-operative treatment options, surgical techniques, and emerging research and clinical developments.GSJ is indexed in PubMedCentral, SCOPUS, and Emerging Sources Citation Index (ESCI).




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
