Implementing a Bedside Percutaneous Tracheostomy and Ultrasound Gastrostomy Team Reduces Length of Stay and Hospital Costs Across Multiple Critical Care Units in a 1500 Bed Tertiary Care Center.
Douglas Houghton, Samarth Patel, Sergey Gerasim, Yaroslav Buryk, Nina Massad, Ayham Alkhachroum, Hany Y Atallah, Kristine O'Phelan
{"title":"Implementing a Bedside Percutaneous Tracheostomy and Ultrasound Gastrostomy Team Reduces Length of Stay and Hospital Costs Across Multiple Critical Care Units in a 1500 Bed Tertiary Care Center.","authors":"Douglas Houghton, Samarth Patel, Sergey Gerasim, Yaroslav Buryk, Nina Massad, Ayham Alkhachroum, Hany Y Atallah, Kristine O'Phelan","doi":"10.1177/08850666241289115","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Thousands of critically ill patients every year in the United States receive tracheostomy and gastrostomy procedures. Recent research has investigated the benefits of a combined team approach to these procedures, with associated decreases in length of stay (LOS) and hospital costs. This study's objective was to determine if implementing a bedside percutaneous tracheostomy and percutaneous ultrasound gastrostomy (PUG) team would reduce LOS and hospital costs. <b>Design and Methods:</b> This retrospective chart review compares the impact of implementing an ICU bedside percutaneous tracheostomy and PUG service team to the hospital's previous workflow (ie, pre-implementation). Inclusion criteria were adult patients with Ventilator Dependent Respiratory Failure (VDRF), a clinical indication for both procedures while admitted to the ICU and received both tracheostomy and gastrostomy procedures while admitted to the hospital. Pre- and post-implementation groups were compared across patients' demographics, clinical characteristics, and outcomes. ICU LOS, hospital LOS and total hospital costs were the primary outcome measures. <b>Results:</b> A total of 101 adult critically ill patients were included in the analysis; 49 patients were in the pre-implementation group and 52 patients in the post-implementation group (ie, PUG group). Patients in the PUG group had a significantly shorter mean ICU LOS and hospital LOS, 10.9- and 14.7-day reductions respectively (p = 0.010, p = 0.006). PUG group patients also had a significant reduction in total hospital costs, a per patient cost savings of $34 778 (p = 0.043). <b>Conclusions:</b> This study supports implementing a bedside percutaneous tracheostomy and PUG team to reduce LOS and total hospital costs in patients with VDRF.</p>","PeriodicalId":16307,"journal":{"name":"Journal of Intensive Care Medicine","volume":" ","pages":"404-409"},"PeriodicalIF":2.1000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12003929/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/08850666241289115","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/22 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
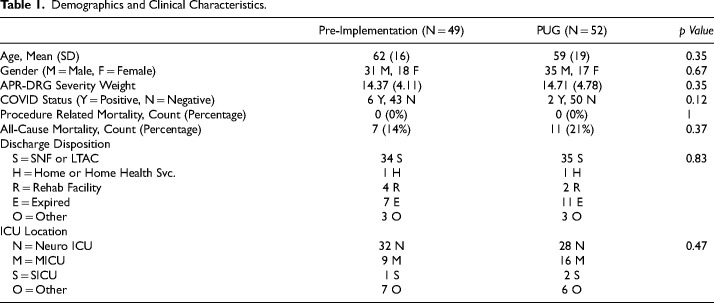
Background: Thousands of critically ill patients every year in the United States receive tracheostomy and gastrostomy procedures. Recent research has investigated the benefits of a combined team approach to these procedures, with associated decreases in length of stay (LOS) and hospital costs. This study's objective was to determine if implementing a bedside percutaneous tracheostomy and percutaneous ultrasound gastrostomy (PUG) team would reduce LOS and hospital costs. Design and Methods: This retrospective chart review compares the impact of implementing an ICU bedside percutaneous tracheostomy and PUG service team to the hospital's previous workflow (ie, pre-implementation). Inclusion criteria were adult patients with Ventilator Dependent Respiratory Failure (VDRF), a clinical indication for both procedures while admitted to the ICU and received both tracheostomy and gastrostomy procedures while admitted to the hospital. Pre- and post-implementation groups were compared across patients' demographics, clinical characteristics, and outcomes. ICU LOS, hospital LOS and total hospital costs were the primary outcome measures. Results: A total of 101 adult critically ill patients were included in the analysis; 49 patients were in the pre-implementation group and 52 patients in the post-implementation group (ie, PUG group). Patients in the PUG group had a significantly shorter mean ICU LOS and hospital LOS, 10.9- and 14.7-day reductions respectively (p = 0.010, p = 0.006). PUG group patients also had a significant reduction in total hospital costs, a per patient cost savings of $34 778 (p = 0.043). Conclusions: This study supports implementing a bedside percutaneous tracheostomy and PUG team to reduce LOS and total hospital costs in patients with VDRF.
期刊介绍:
Journal of Intensive Care Medicine (JIC) is a peer-reviewed bi-monthly journal offering medical and surgical clinicians in adult and pediatric intensive care state-of-the-art, broad-based analytic reviews and updates, original articles, reports of large clinical series, techniques and procedures, topic-specific electronic resources, book reviews, and editorials on all aspects of intensive/critical/coronary care.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
