Stroke-heart syndrome and early mortality in patients with acute ischaemic stroke using hierarchical cluster analysis: An individual patient data pooled analysis from the VISTA database.
Hironori Ishiguchi, Bi Huang, Wahbi K El-Bouri, Gregory Y H Lip, Azmil H Abdul-Rahim
{"title":"Stroke-heart syndrome and early mortality in patients with acute ischaemic stroke using hierarchical cluster analysis: An individual patient data pooled analysis from the VISTA database.","authors":"Hironori Ishiguchi, Bi Huang, Wahbi K El-Bouri, Gregory Y H Lip, Azmil H Abdul-Rahim","doi":"10.1177/23969873241290440","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The patient clinical phenotypes at particularly high risk for early cardiac complications after a recent acute ischaemic stroke (AIS), that is, stroke-heart syndrome (SHS), remain poorly defined. We utilised hierarchical cluster analysis to identify specific phenotypic profiles associated with this risk.</p><p><strong>Methods: </strong>We gathered data on patients with AIS from the Virtual International Stroke Trials Archive, a global repository of clinical trial data. We examined cardiac complications within 30 days post-stroke, including acute coronary syndrome, heart failure, arrhythmias and cardiorespiratory arrest. We employed hierarchical cluster analysis to define distinct phenotypic risk profiles. The incidence/risk of SHS and 90-day mortality were compared across these profiles.</p><p><strong>Results: </strong>We included 12,482 patients (mean age 69 ± 12 years; 55% male), yielding five phenotypes: Profile 1 ('<i>elderly and AF</i>'), Profile 2 ('<i>young and smoker</i>'), Profile 3 ('<i>young</i>'), Profile 4 ('<i>cardiac comorbidities</i>') and Profile 5 ('<i>hypertension with atherosclerotic comorbidities</i>'). Profiles 4 and 1 exhibited the highest risk for SHS (adjusted HR (95% CI): 2.01 (1.70-2.38) and 1.26 (1.05-1.51), respectively, compared to Profile 3), while Profiles 5 and 2 showed moderate risk and Profile 3 had the lowest risk. Although Profiles 1 and 4 were at the highest risk for most SHS presentations, Profile 5 had the highest risk for cardiorespiratory arrest (adjusted HR (95% CI): 2.99 (1.22-7.34)). The 90-day mortality risk was stratified by phenotype, with the highest risk observed in Profiles 5, and 4.</p><p><strong>Conclusions: </strong>Hierarchical cluster analysis effectively identified phenotypes with the highest risk of SHS and early mortality in patients with AIS.</p>","PeriodicalId":46821,"journal":{"name":"European Stroke Journal","volume":" ","pages":"478-486"},"PeriodicalIF":4.5000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11556556/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Stroke Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/23969873241290440","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/13 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The patient clinical phenotypes at particularly high risk for early cardiac complications after a recent acute ischaemic stroke (AIS), that is, stroke-heart syndrome (SHS), remain poorly defined. We utilised hierarchical cluster analysis to identify specific phenotypic profiles associated with this risk.
Methods: We gathered data on patients with AIS from the Virtual International Stroke Trials Archive, a global repository of clinical trial data. We examined cardiac complications within 30 days post-stroke, including acute coronary syndrome, heart failure, arrhythmias and cardiorespiratory arrest. We employed hierarchical cluster analysis to define distinct phenotypic risk profiles. The incidence/risk of SHS and 90-day mortality were compared across these profiles.
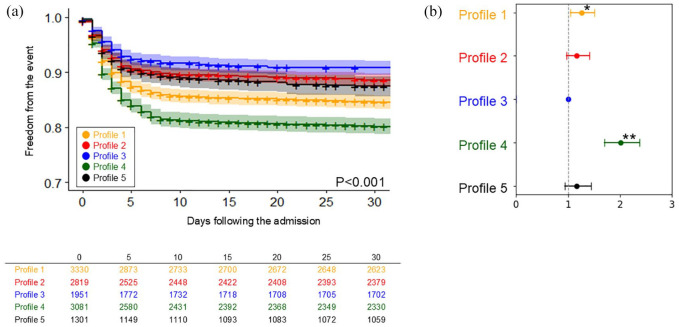
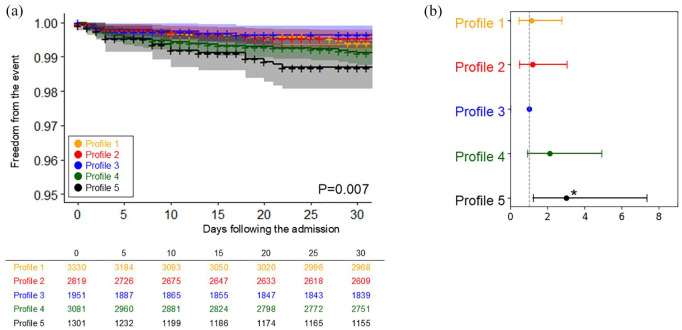
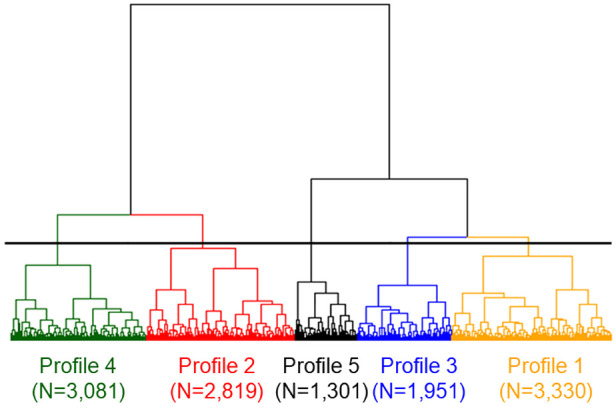
Results: We included 12,482 patients (mean age 69 ± 12 years; 55% male), yielding five phenotypes: Profile 1 ('elderly and AF'), Profile 2 ('young and smoker'), Profile 3 ('young'), Profile 4 ('cardiac comorbidities') and Profile 5 ('hypertension with atherosclerotic comorbidities'). Profiles 4 and 1 exhibited the highest risk for SHS (adjusted HR (95% CI): 2.01 (1.70-2.38) and 1.26 (1.05-1.51), respectively, compared to Profile 3), while Profiles 5 and 2 showed moderate risk and Profile 3 had the lowest risk. Although Profiles 1 and 4 were at the highest risk for most SHS presentations, Profile 5 had the highest risk for cardiorespiratory arrest (adjusted HR (95% CI): 2.99 (1.22-7.34)). The 90-day mortality risk was stratified by phenotype, with the highest risk observed in Profiles 5, and 4.
Conclusions: Hierarchical cluster analysis effectively identified phenotypes with the highest risk of SHS and early mortality in patients with AIS.
期刊介绍:
Launched in 2016 the European Stroke Journal (ESJ) is the official journal of the European Stroke Organisation (ESO), a professional non-profit organization with over 1,400 individual members, and affiliations to numerous related national and international societies. ESJ covers clinical stroke research from all fields, including clinical trials, epidemiology, primary and secondary prevention, diagnosis, acute and post-acute management, guidelines, translation of experimental findings into clinical practice, rehabilitation, organisation of stroke care, and societal impact. It is open to authors from all relevant medical and health professions. Article types include review articles, original research, protocols, guidelines, editorials and letters to the Editor. Through ESJ, authors and researchers have gained a new platform for the rapid and professional publication of peer reviewed scientific material of the highest standards; publication in ESJ is highly competitive. The journal and its editorial team has developed excellent cooperation with sister organisations such as the World Stroke Organisation and the International Journal of Stroke, and the American Heart Organization/American Stroke Association and the journal Stroke. ESJ is fully peer-reviewed and is a member of the Committee on Publication Ethics (COPE). Issues are published 4 times a year (March, June, September and December) and articles are published OnlineFirst prior to issue publication.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
