Gabriele M. Iacona MD , Jules J. Bakhos MD, MSc , Penny L. Houghtaling MS , Aaron E. Tipton MD , Richard Ramsingh MD , Nicholas G. Smedira MD , Marc Gillinov MD , Kenneth R. McCurry MD , Edward G. Soltesz MD , Eric E. Roselli MD , Michael Z. Tong MD , Shinya G. Unai MD , Haytham J. Elgharably MD , Marijan J. Koprivanac MD , Lars G. Svensson MD, PhD , Eugene H. Blackstone MD , Faisal G. Bakaeen MD
{"title":"Multiarterial grafting in redo coronary artery bypass grafting: Type of arterial conduit and patient sex determine benefit","authors":"Gabriele M. Iacona MD , Jules J. Bakhos MD, MSc , Penny L. Houghtaling MS , Aaron E. Tipton MD , Richard Ramsingh MD , Nicholas G. Smedira MD , Marc Gillinov MD , Kenneth R. McCurry MD , Edward G. Soltesz MD , Eric E. Roselli MD , Michael Z. Tong MD , Shinya G. Unai MD , Haytham J. Elgharably MD , Marijan J. Koprivanac MD , Lars G. Svensson MD, PhD , Eugene H. Blackstone MD , Faisal G. Bakaeen MD","doi":"10.1016/j.jtcvs.2024.10.018","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><div><span>To evaluate whether multiarterial grafting provides an incremental benefit above single arterial grafting in isolated redo </span>coronary artery bypass grafting (CABG).</div></div><div><h3>Methods</h3><div>From January 1980 to July 2020, 6559 adults underwent a total of 6693 isolated CABG reoperations<span><span>. Patients undergoing multiarterial grafting were propensity score–matched with those undergoing single arterial grafting with or without additional vein grafts, yielding 2005 well-matched pairs. Endpoints were in-hospital </span>postoperative complications, hospital mortality, and long-term mortality. The median follow-up was 10 years, with 25% of patients followed for >17 years. Multivariable multiphase hazard models and nonparametric random survival forest models for survival were used to identify patients for whom multiarterial grafting was most beneficial.</span></div></div><div><h3>Results</h3><div><span>Among propensity score–matched patients, postoperative complications in multiarterial versus single arterial grafting included any reoperation (50 [2.5%] vs 65 [3.2%]); renal failure (73 [3.6%] vs 55 [2.7%]), stroke (44 [2.2%] vs 38 [1.9%]), and deep sternal infection (36 [1.8%] vs 25 [1.2%]). In-hospital mortality was 1.7% (n = 35) in multiarterial grafting versus 2.8% (n = 56) in single arterial grafting (</span><em>P</em><span> = .03). Comparing multiarterial to single arterial grafting, overall survival<span> was 95% versus 94% at 1 year, 92% versus 88% at 3 years, 87% versus 82% at 5 years, 49% versus 42% at 15 years, and 31% versus 25% at 20 years. Better survival after multiarterial grafting was confined to males with 2 patent internal thoracic artery grafts (</span></span><em>P</em> < .0001).</div></div><div><h3>Conclusions</h3><div>Redo CABG with multiarterial grafting can be performed with lower in-hospital mortality and similar major morbidity to single arterial grafting. It is associated with better long-term survival, particularly in males when 2 internal thoracic artery grafts are used.</div></div>","PeriodicalId":49975,"journal":{"name":"Journal of Thoracic and Cardiovascular Surgery","volume":"170 4","pages":"Pages 1079-1086.e6"},"PeriodicalIF":4.4000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0022522324009279","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/18 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
To evaluate whether multiarterial grafting provides an incremental benefit above single arterial grafting in isolated redo coronary artery bypass grafting (CABG).
Methods
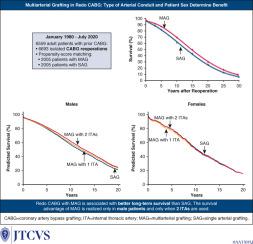
From January 1980 to July 2020, 6559 adults underwent a total of 6693 isolated CABG reoperations. Patients undergoing multiarterial grafting were propensity score–matched with those undergoing single arterial grafting with or without additional vein grafts, yielding 2005 well-matched pairs. Endpoints were in-hospital postoperative complications, hospital mortality, and long-term mortality. The median follow-up was 10 years, with 25% of patients followed for >17 years. Multivariable multiphase hazard models and nonparametric random survival forest models for survival were used to identify patients for whom multiarterial grafting was most beneficial.
Results
Among propensity score–matched patients, postoperative complications in multiarterial versus single arterial grafting included any reoperation (50 [2.5%] vs 65 [3.2%]); renal failure (73 [3.6%] vs 55 [2.7%]), stroke (44 [2.2%] vs 38 [1.9%]), and deep sternal infection (36 [1.8%] vs 25 [1.2%]). In-hospital mortality was 1.7% (n = 35) in multiarterial grafting versus 2.8% (n = 56) in single arterial grafting (P = .03). Comparing multiarterial to single arterial grafting, overall survival was 95% versus 94% at 1 year, 92% versus 88% at 3 years, 87% versus 82% at 5 years, 49% versus 42% at 15 years, and 31% versus 25% at 20 years. Better survival after multiarterial grafting was confined to males with 2 patent internal thoracic artery grafts (P < .0001).
Conclusions
Redo CABG with multiarterial grafting can be performed with lower in-hospital mortality and similar major morbidity to single arterial grafting. It is associated with better long-term survival, particularly in males when 2 internal thoracic artery grafts are used.
期刊介绍:
The Journal of Thoracic and Cardiovascular Surgery presents original, peer-reviewed articles on diseases of the heart, great vessels, lungs and thorax with emphasis on surgical interventions. An official publication of The American Association for Thoracic Surgery and The Western Thoracic Surgical Association, the Journal focuses on techniques and developments in acquired cardiac surgery, congenital cardiac repair, thoracic procedures, heart and lung transplantation, mechanical circulatory support and other procedures.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
