Michael J. Burla DO, Peter C. Michalakes BA, Jeanne S. Wishengrad MSc, Drew R. York BA, Holly A. Stevens BSN-RN,MHRT-CSP, Teresa L. May DO
{"title":"Assessing variations in care delivered to rural out of hospital cardiac arrest patients in the interfacility transfer setting","authors":"Michael J. Burla DO, Peter C. Michalakes BA, Jeanne S. Wishengrad MSc, Drew R. York BA, Holly A. Stevens BSN-RN,MHRT-CSP, Teresa L. May DO","doi":"10.1002/emp2.13330","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objective</h3>\n \n <p>There is significant variation in out-of-hospital cardiac arrest (OHCA) outcomes between different regions. We sought to evaluate outcomes of OHCA patients in the interfacility transfer (IFT) setting, between critical care transport (LifeFlight) and community Emergency Medical Services (EMS), in the state of Maine.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This was a retrospective analysis of our institution's electronic medical record and the Maine EMS database. Data were collected from January 1, 2019, to December 31, 2021. Only adult OHCA encounters requiring an IFT for definitive post-cardiac-arrest care were included. Demographics, EMS agency, IFT vital signs, targeted temperature management (TTM) medications, cerebral performance category (CPC) scores, survival to discharge, and other descriptive variables were collected.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Ninety-three patients met inclusion criteria, with LifeFlight transferring 30 of them (32.3%). LifeFlight was more likely to initiate TTM compared to other EMS agencies (<i>p</i> = 0.012), have run-sheets reported (<i>p</i> = 0.001), and serve rural areas (<i>p</i> = 0.036). LifeFlight was associated with more epinephrine (0.034) and norepinephrine (<0.001) use. Only 37% of IFTs had physician orders, with none (0.0%) of them defining vital sign targets. No difference in survival to discharge or CPC scores was observed between LifeFlight and other EMS agencies. No significant variation in comorbidities or vital signs was observed.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>There was no difference in survival to discharge or CPC scores between LifeFlight and ad hoc EMS agency. LifeFlight was associated with more TTM and vasopressor utilization during IFT. Most IFT encounters did not have dedicated physician orders, and none of the orders included vital sign targets.</p>\n </section>\n </div>","PeriodicalId":73967,"journal":{"name":"Journal of the American College of Emergency Physicians open","volume":"5 5","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11491542/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Emergency Physicians open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13330","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
There is significant variation in out-of-hospital cardiac arrest (OHCA) outcomes between different regions. We sought to evaluate outcomes of OHCA patients in the interfacility transfer (IFT) setting, between critical care transport (LifeFlight) and community Emergency Medical Services (EMS), in the state of Maine.
Methods
This was a retrospective analysis of our institution's electronic medical record and the Maine EMS database. Data were collected from January 1, 2019, to December 31, 2021. Only adult OHCA encounters requiring an IFT for definitive post-cardiac-arrest care were included. Demographics, EMS agency, IFT vital signs, targeted temperature management (TTM) medications, cerebral performance category (CPC) scores, survival to discharge, and other descriptive variables were collected.
Results
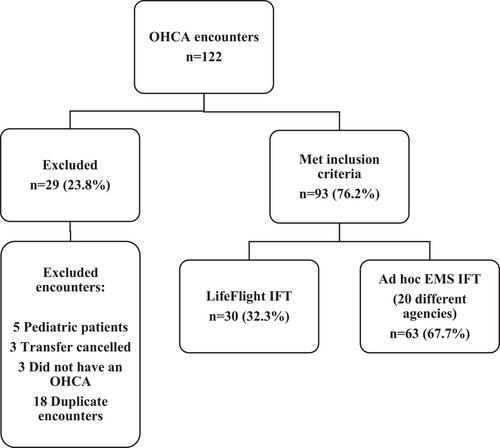
Ninety-three patients met inclusion criteria, with LifeFlight transferring 30 of them (32.3%). LifeFlight was more likely to initiate TTM compared to other EMS agencies (p = 0.012), have run-sheets reported (p = 0.001), and serve rural areas (p = 0.036). LifeFlight was associated with more epinephrine (0.034) and norepinephrine (<0.001) use. Only 37% of IFTs had physician orders, with none (0.0%) of them defining vital sign targets. No difference in survival to discharge or CPC scores was observed between LifeFlight and other EMS agencies. No significant variation in comorbidities or vital signs was observed.
Conclusions
There was no difference in survival to discharge or CPC scores between LifeFlight and ad hoc EMS agency. LifeFlight was associated with more TTM and vasopressor utilization during IFT. Most IFT encounters did not have dedicated physician orders, and none of the orders included vital sign targets.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
