{"title":"A Comprehensive Nomogram Integrating Phonocardiogram and Echocardiogram Features for the Diagnosis of Heart Failure With Preserved Ejection Fraction","authors":"Linchun Cao, Xingming Guo, Kangla Liao, Jian Qin, Yineng Zheng","doi":"10.1002/clc.70022","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Heart failure with preserved ejection fraction (HFpEF) is associated with high hospitalization and mortality rates, representing a significant healthcare burden. This study aims to utilize various information including echocardiogram and phonocardiogram to construct and validate a nomogram, assisting in clinical decision-making.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This study analyzed 204 patients (68 HFpEF and 136 non-HFpEF) from the First Affiliated Hospital of Chongqing Medical University. A total of 49 features were integrated and used, including phonocardiogram, echocardiogram features, and clinical parameters. The least absolute shrinkage and selection operator (LASSO) regression was used to select the optimal matching factors, and a stepwise logistic regression was employed to determine independent risk factors and develop a nomogram. Model performance was evaluated by the area under receiver operating characteristic (ROC) curve (AUC), calibration curve, decision curve analysis (DCA), and clinical impact curve (CIC).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The nomogram was constructed using five significant indicators, including NT-proBNP (OR = 4.689, <i>p</i> = 0.015), <i>E</i>/<i>e</i>′ (OR = 1.219, <i>p</i> = 0.032), LAVI (OR = 1.088, <i>p</i> < 0.01), D/S (OR = 0.014, <i>p</i> < 0.01), and QM1 (OR = 1.058, <i>p</i> < 0.01), and showed a better AUC of 0.945 (95% CI = 0.908–0.982) in the training set and 0.933 (95% CI = 0.873–0.992) in the testing set compared to conventional nomogram without phonocardiogram features. The calibration curve and Hosmer–Lemeshow test demonstrated no statistical significance in the training and testing sets (<i>p</i> = 0.814 and <i>p</i> = 0.736), indicating the nomogram was well-calibrated. The DCA and CIC results confirmed favorable clinical usefulness.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>The nomogram, integrating phonocardiogram and echocardiogram features, enhances HFpEF diagnostic efficiency, offering a valuable tool for clinical decision-making.</p>\n </section>\n </div>","PeriodicalId":10201,"journal":{"name":"Clinical Cardiology","volume":"47 11","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2024-10-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.70022","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Cardiology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clc.70022","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Heart failure with preserved ejection fraction (HFpEF) is associated with high hospitalization and mortality rates, representing a significant healthcare burden. This study aims to utilize various information including echocardiogram and phonocardiogram to construct and validate a nomogram, assisting in clinical decision-making.
Methods
This study analyzed 204 patients (68 HFpEF and 136 non-HFpEF) from the First Affiliated Hospital of Chongqing Medical University. A total of 49 features were integrated and used, including phonocardiogram, echocardiogram features, and clinical parameters. The least absolute shrinkage and selection operator (LASSO) regression was used to select the optimal matching factors, and a stepwise logistic regression was employed to determine independent risk factors and develop a nomogram. Model performance was evaluated by the area under receiver operating characteristic (ROC) curve (AUC), calibration curve, decision curve analysis (DCA), and clinical impact curve (CIC).
Results
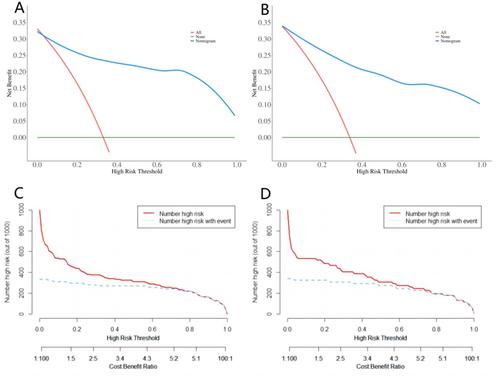
The nomogram was constructed using five significant indicators, including NT-proBNP (OR = 4.689, p = 0.015), E/e′ (OR = 1.219, p = 0.032), LAVI (OR = 1.088, p < 0.01), D/S (OR = 0.014, p < 0.01), and QM1 (OR = 1.058, p < 0.01), and showed a better AUC of 0.945 (95% CI = 0.908–0.982) in the training set and 0.933 (95% CI = 0.873–0.992) in the testing set compared to conventional nomogram without phonocardiogram features. The calibration curve and Hosmer–Lemeshow test demonstrated no statistical significance in the training and testing sets (p = 0.814 and p = 0.736), indicating the nomogram was well-calibrated. The DCA and CIC results confirmed favorable clinical usefulness.
Conclusion
The nomogram, integrating phonocardiogram and echocardiogram features, enhances HFpEF diagnostic efficiency, offering a valuable tool for clinical decision-making.
期刊介绍:
Clinical Cardiology provides a fully Gold Open Access forum for the publication of original clinical research, as well as brief reviews of diagnostic and therapeutic issues in cardiovascular medicine and cardiovascular surgery.
The journal includes Clinical Investigations, Reviews, free standing editorials and commentaries, and bonus online-only content.
The journal also publishes supplements, Expert Panel Discussions, sponsored clinical Reviews, Trial Designs, and Quality and Outcomes.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
