Fawaz Altuwaijri, Abdulaziz Alrabiah, Abdullah Alqarni, Alia Kamal Habash, Mohammad Alghofili, Omar Alotaibi, Mansour Altuwaijri
{"title":"Comparison Between the Advanced Cardiac Life Support and Adult Advanced Life Support Protocols: A Simulation-Based Pilot Study.","authors":"Fawaz Altuwaijri, Abdulaziz Alrabiah, Abdullah Alqarni, Alia Kamal Habash, Mohammad Alghofili, Omar Alotaibi, Mansour Altuwaijri","doi":"10.1155/2024/6696879","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction:</b> Cardiac arrest is a public health concern associated with unfavorable disease outcomes. Cardiopulmonary resuscitation (CPR) of optimal quality is widely acknowledged as an indispensable technique in restoring spontaneous circulation. In order to perform advanced cardiac life support (ACLS), chest compression must be paused twice: once to assess the rhythm and again to administer the shock. Australian advanced life support (ALS) recommends that the defibrillator needs to be precharged in order to administer the shock during a solitary interval in chest compressions. While performing chest compressions, precharging defibrillators can decrease hands-off time without posing a risk of injury. <b>Aim:</b> To compare chest compression fraction (CCF)-which is the cumulative time spent providing chest compressions divided by the total time taken for the entire resuscitation-by calculating the hands-off time duration in cardiac arrest between the Australian Resuscitation Council (ARC) and American Heart Association (AHA) protocols for CPR. <b>Methods:</b> A simulation-based pilot study was designed using a Laerdal Resusci Anne mannequin and a LIFEPACK 20 defibrillator. The study included six participants recruited from King Khalid University Hospital in Riyadh, Saudi Arabia, where three participants were certified ACLS providers and there were certified ALS providers. Participants were divided into two groups, ALS and ACLS, each following one protocol. For each scenario, a random job was assigned to each participant, regardless of their role as assistant, team leader, or performer of CPR. Each case's shockable and nonshockable rhythms were hidden from the team leader and the chest compressor. Ten trials of CPR were performed, each for four cycles with a total time of 8 min. The simulation was video recorded for hands-off time counting. Comparison between CCF (seconds) per cycle between the two protocols was performed using an independent sample <i>t</i>-test. A <i>p</i> value of 0.05 was used to measure statistical significance. <b>Results:</b> Comparing CCF in shockable rhythms between ARC and AHA protocols, it was observed that the CCF of ALS-ARC was significantly higher than ACLS-AHA in all cycles; the first cycle: <i>t</i> = 3.782, <i>p</i>=0.004; the second cycle: <i>t</i> = 3.380, <i>p</i>=0.007; the third cycle: <i>t</i> = 3.803, <i>p</i>=0.003; and the fourth cycle: <i>t</i> = 4.341, <i>p</i>=0.001. <b>Conclusion:</b> Precharging a defibrillator before a rhythm check during chest compression, in anticipation of a potentially shockable rhythm, reduces the time required for defibrillation and limits interruptions in chest compression during CPR. This practice effectively enhances the CCF. Enhancing the continuity of chest compressions can potentially improve survival rates in ARC.</p>","PeriodicalId":11528,"journal":{"name":"Emergency Medicine International","volume":"2024 ","pages":"6696879"},"PeriodicalIF":0.8000,"publicationDate":"2024-10-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11511593/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Emergency Medicine International","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2024/6696879","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
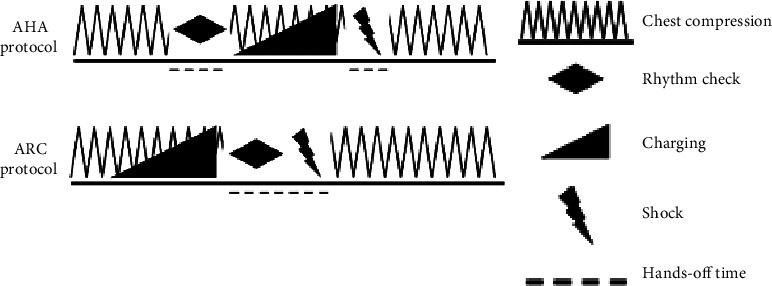
Introduction: Cardiac arrest is a public health concern associated with unfavorable disease outcomes. Cardiopulmonary resuscitation (CPR) of optimal quality is widely acknowledged as an indispensable technique in restoring spontaneous circulation. In order to perform advanced cardiac life support (ACLS), chest compression must be paused twice: once to assess the rhythm and again to administer the shock. Australian advanced life support (ALS) recommends that the defibrillator needs to be precharged in order to administer the shock during a solitary interval in chest compressions. While performing chest compressions, precharging defibrillators can decrease hands-off time without posing a risk of injury. Aim: To compare chest compression fraction (CCF)-which is the cumulative time spent providing chest compressions divided by the total time taken for the entire resuscitation-by calculating the hands-off time duration in cardiac arrest between the Australian Resuscitation Council (ARC) and American Heart Association (AHA) protocols for CPR. Methods: A simulation-based pilot study was designed using a Laerdal Resusci Anne mannequin and a LIFEPACK 20 defibrillator. The study included six participants recruited from King Khalid University Hospital in Riyadh, Saudi Arabia, where three participants were certified ACLS providers and there were certified ALS providers. Participants were divided into two groups, ALS and ACLS, each following one protocol. For each scenario, a random job was assigned to each participant, regardless of their role as assistant, team leader, or performer of CPR. Each case's shockable and nonshockable rhythms were hidden from the team leader and the chest compressor. Ten trials of CPR were performed, each for four cycles with a total time of 8 min. The simulation was video recorded for hands-off time counting. Comparison between CCF (seconds) per cycle between the two protocols was performed using an independent sample t-test. A p value of 0.05 was used to measure statistical significance. Results: Comparing CCF in shockable rhythms between ARC and AHA protocols, it was observed that the CCF of ALS-ARC was significantly higher than ACLS-AHA in all cycles; the first cycle: t = 3.782, p=0.004; the second cycle: t = 3.380, p=0.007; the third cycle: t = 3.803, p=0.003; and the fourth cycle: t = 4.341, p=0.001. Conclusion: Precharging a defibrillator before a rhythm check during chest compression, in anticipation of a potentially shockable rhythm, reduces the time required for defibrillation and limits interruptions in chest compression during CPR. This practice effectively enhances the CCF. Enhancing the continuity of chest compressions can potentially improve survival rates in ARC.
期刊介绍:
Emergency Medicine International is a peer-reviewed, Open Access journal that provides a forum for doctors, nurses, paramedics and ambulance staff. The journal publishes original research articles, review articles, and clinical studies related to prehospital care, disaster preparedness and response, acute medical and paediatric emergencies, critical care, sports medicine, wound care, and toxicology.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
