{"title":"Comparing Cesarean Scar Defect Incidence After Locked and Unlocked Repair Methods Among Primiparous Patients: A Randomized Double-Blinded Trial.","authors":"Azadeh Tarafdari, Mahdieh Nazarpour, Nikan Zargardzadeh, Sedigheh Hantoushzadeh, Mohammadamin Parsaei","doi":"10.18502/jfrh.v18i3.16655","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To compare residual myometrial thickness (RMT) and cesarean scar defect (CSD) development after cesarean section using double-layer locked and unlocked closure techniques.</p><p><strong>Materials and methods: </strong>We conducted a randomized double-blinded trial comparing double-layer locked and unlocked uterine closure techniques following cesarean section in primiparous women. The locked technique involved continuous suturing of the full myometrial thickness in the first layer, followed by back-and-forth needle maneuvering on both sides of the incision for the second layer. The unlocked method included running suturing of two-thirds of the myometrial thickness in the first layer, followed by suturing the upper half of the myometrial thickness in the second layer. Transvaginal ultrasonography was performed one year post-cesarean section, with RMT as the primary outcome and scar depth and width as secondary outcomes. Independent t-test and Chi-square test were utilized for statistical analysis.</p><p><strong>Results: </strong>All 30 patients from the locked and 26 from the unlocked group in the follow-up were diagnosed with CSD (scar depth>2mm). The mean RMT for the unlocked and locked groups were 4.44±1.07mm and 4.12±0.48mm, respectively, showing no significant difference (p =0.14). There was also no significant difference in mean scar width between the locked and unlocked groups (3.68±1.44mm vs. 3.95±1.00mm, p =0.42). However, the mean scar depth was higher in the unlocked group (3.77±1.11 mm vs. 3.16±1.1mm, p =0.04).</p><p><strong>Conclusion: </strong>We have found no significant differences in the RMT and CSD prevalence between two-layered locked and unlocked uterine closure techniques, while the scar depth was greater in the unlocked group. Nonetheless, future randomized trials implementing larger sample sizes are required to precisely compare the outcomes of the double-layer locked and unlocked uterine suturing techniques.</p>","PeriodicalId":15845,"journal":{"name":"Journal of Family and Reproductive Health","volume":"18 3","pages":"146-153"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11491697/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Family and Reproductive Health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18502/jfrh.v18i3.16655","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To compare residual myometrial thickness (RMT) and cesarean scar defect (CSD) development after cesarean section using double-layer locked and unlocked closure techniques.
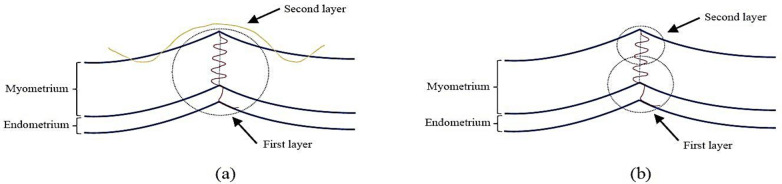
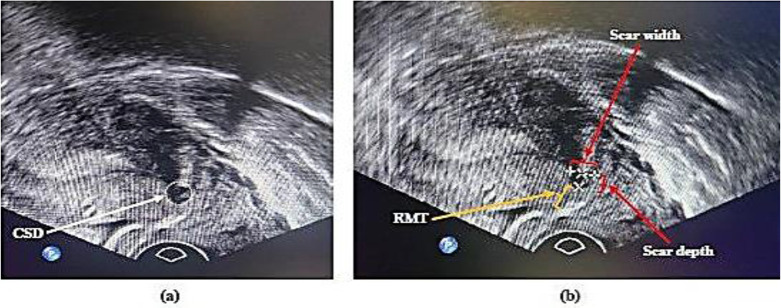
Materials and methods: We conducted a randomized double-blinded trial comparing double-layer locked and unlocked uterine closure techniques following cesarean section in primiparous women. The locked technique involved continuous suturing of the full myometrial thickness in the first layer, followed by back-and-forth needle maneuvering on both sides of the incision for the second layer. The unlocked method included running suturing of two-thirds of the myometrial thickness in the first layer, followed by suturing the upper half of the myometrial thickness in the second layer. Transvaginal ultrasonography was performed one year post-cesarean section, with RMT as the primary outcome and scar depth and width as secondary outcomes. Independent t-test and Chi-square test were utilized for statistical analysis.
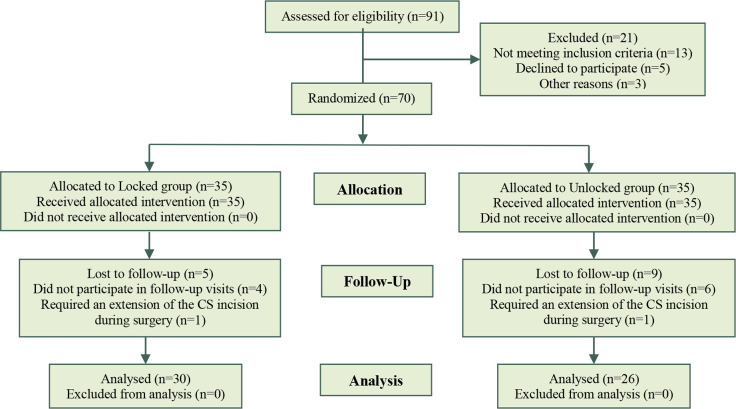
Results: All 30 patients from the locked and 26 from the unlocked group in the follow-up were diagnosed with CSD (scar depth>2mm). The mean RMT for the unlocked and locked groups were 4.44±1.07mm and 4.12±0.48mm, respectively, showing no significant difference (p =0.14). There was also no significant difference in mean scar width between the locked and unlocked groups (3.68±1.44mm vs. 3.95±1.00mm, p =0.42). However, the mean scar depth was higher in the unlocked group (3.77±1.11 mm vs. 3.16±1.1mm, p =0.04).
Conclusion: We have found no significant differences in the RMT and CSD prevalence between two-layered locked and unlocked uterine closure techniques, while the scar depth was greater in the unlocked group. Nonetheless, future randomized trials implementing larger sample sizes are required to precisely compare the outcomes of the double-layer locked and unlocked uterine suturing techniques.
期刊介绍:
The Journal of Family & Reproductive Health (JFRH) is the quarterly official journal of Vali–e–Asr Reproductive Health Research Center. This journal features fulllength, peerreviewed papers reporting original research, clinical case histories, review articles, as well as opinions and debates on topical issues. Papers published cover the scientific and medical aspects of reproductive physiology and pathology including genetics, endocrinology, andrology, embryology, gynecologic urology, fetomaternal medicine, oncology, infectious disease, public health, nutrition, surgery, menopause, family planning, infertility, psychiatry–psychology, demographic modeling, perinatalogy–neonatolgy ethics and social issues, and pharmacotherapy. A high scientific and editorial standard is maintained throughout the journal along with a regular rate of publication. All published articles will become the property of the JFRH. The editor and publisher accept no responsibility for the statements expressed by the authors here in. Also they do not guarantee, warrant or endorse any product or service advertised in the journal.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
