Optimizing muscle preservation during weight loss in patients with cirrhosis: A pilot study comparing continuous energy restriction to alternate-day modified fasting for weight loss in patients with obesity and non-alcoholic cirrhosis of the liver.
Winston Dunn, Stephen D Herrmann, Robert N Montgomery, Mary Hastert, Jeffery J Honas, Jessica Rachman, Joseph E Donnelly, Felicia L Steger
{"title":"Optimizing muscle preservation during weight loss in patients with cirrhosis: A pilot study comparing continuous energy restriction to alternate-day modified fasting for weight loss in patients with obesity and non-alcoholic cirrhosis of the liver.","authors":"Winston Dunn, Stephen D Herrmann, Robert N Montgomery, Mary Hastert, Jeffery J Honas, Jessica Rachman, Joseph E Donnelly, Felicia L Steger","doi":"10.1002/osp4.70016","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Obesity is associated with increased morbidity in patients with advanced liver disease, but it is particularly challenging for these patients to preserve skeletal muscle mass during weight loss and accelerating sarcopenia is a concern. Alternate-day modified fasting (ADMF) may be particularly effective for weight loss in patients with concomitant cirrhosis and obesity due to preservation of fat-free mass (FFM).</p><p><strong>Methods: </strong>A weight loss program featuring either ADMF or a continuous low-calorie diet (LCD) was evaluated in a 24-week randomized clinical trial in 20 adult patients with Child-Pugh Class A cirrhosis and obesity. Participants were randomized to either ADMF (<i>n</i> = 11) or LCD (<i>n</i> = 9). Both groups received a remotely delivered exercise program. Body composition, sarcopenia measures, and functional outcomes were assessed pre-post.</p><p><strong>Results: </strong>Thirteen participants completed the intervention (Age = 57 ± 10; BMI = 37.7 ± 5.8 kg/m<sup>2</sup>). The median body weight lost in ADMF was 13.7 ± 4.8 kg (13.9% of initial body weight), while LCD lost 9.9 ± 6.9 kg (10.7% of initial body weight). Total body fat percentage decreased in both groups (ADMF: -4.1 ± 4.0%; LCD = -2.8 ± 1.4%). Fat-free mass accounted for 34 ± 20% of total weight loss in ADMF and 38 ± 10% in LCD. Functional measures, such as timed chair stands, improved in both groups.</p><p><strong>Conclusion: </strong>This pilot study demonstrates the feasibility of the ADMF and LCD interventions to produce significant weight loss while improving body composition in patients with cirrhosis and obesity. Further research is needed to validate these findings in larger cohorts and to assess changes in muscle quality and visceral fat.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov Identifier: NCT05367596.</p>","PeriodicalId":19448,"journal":{"name":"Obesity Science & Practice","volume":"10 5","pages":"e70016"},"PeriodicalIF":1.9000,"publicationDate":"2024-10-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11500757/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Obesity Science & Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/osp4.70016","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Obesity is associated with increased morbidity in patients with advanced liver disease, but it is particularly challenging for these patients to preserve skeletal muscle mass during weight loss and accelerating sarcopenia is a concern. Alternate-day modified fasting (ADMF) may be particularly effective for weight loss in patients with concomitant cirrhosis and obesity due to preservation of fat-free mass (FFM).
Methods: A weight loss program featuring either ADMF or a continuous low-calorie diet (LCD) was evaluated in a 24-week randomized clinical trial in 20 adult patients with Child-Pugh Class A cirrhosis and obesity. Participants were randomized to either ADMF (n = 11) or LCD (n = 9). Both groups received a remotely delivered exercise program. Body composition, sarcopenia measures, and functional outcomes were assessed pre-post.
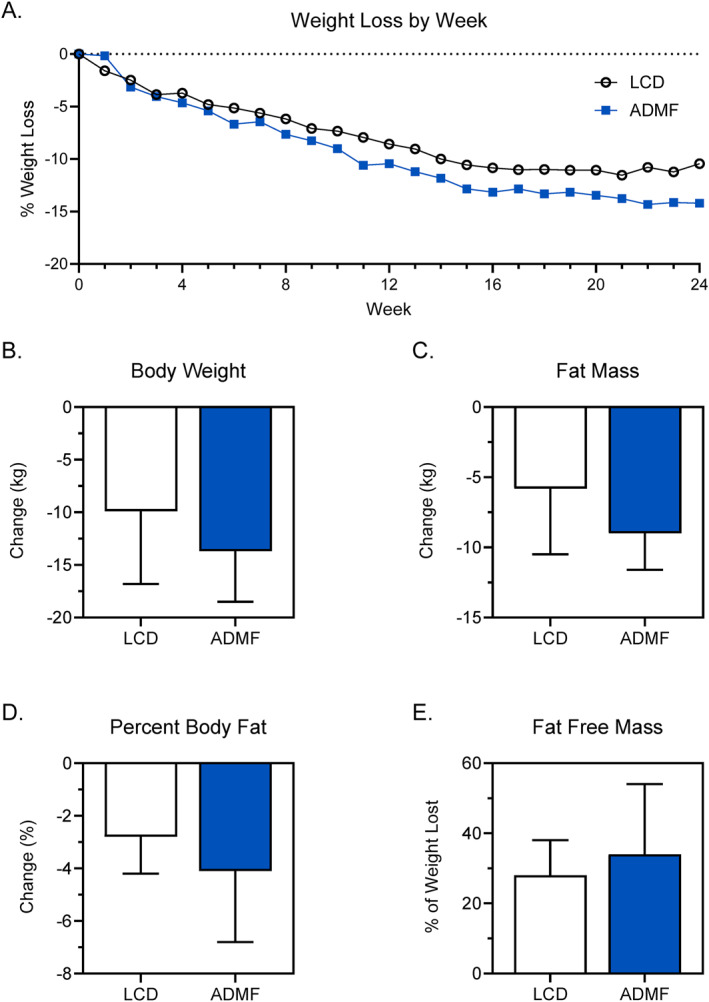
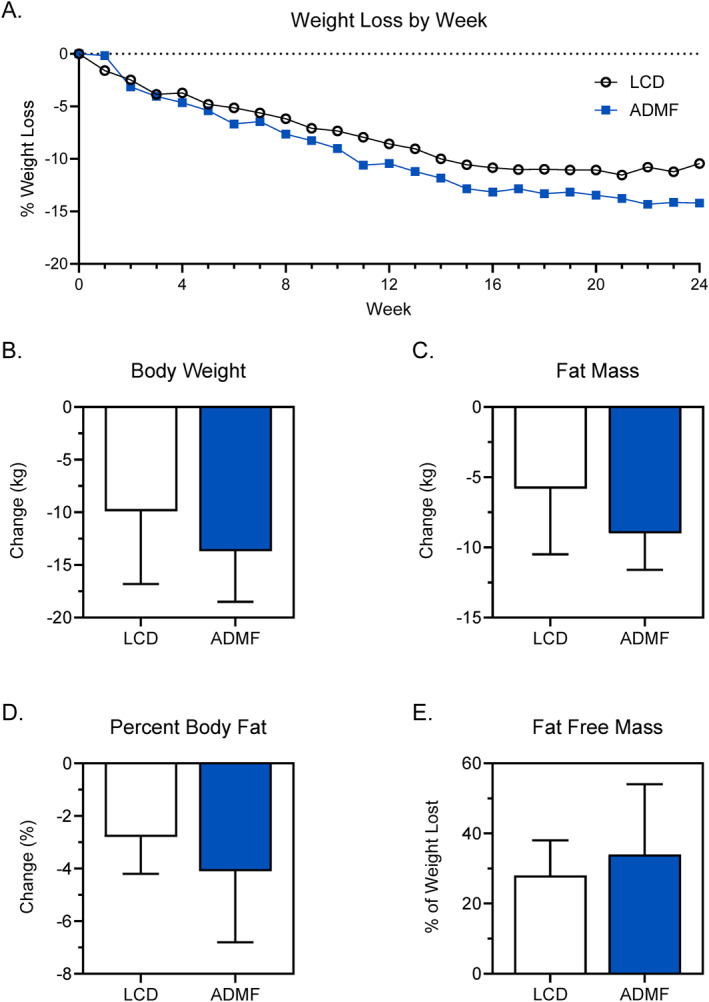
Results: Thirteen participants completed the intervention (Age = 57 ± 10; BMI = 37.7 ± 5.8 kg/m2). The median body weight lost in ADMF was 13.7 ± 4.8 kg (13.9% of initial body weight), while LCD lost 9.9 ± 6.9 kg (10.7% of initial body weight). Total body fat percentage decreased in both groups (ADMF: -4.1 ± 4.0%; LCD = -2.8 ± 1.4%). Fat-free mass accounted for 34 ± 20% of total weight loss in ADMF and 38 ± 10% in LCD. Functional measures, such as timed chair stands, improved in both groups.
Conclusion: This pilot study demonstrates the feasibility of the ADMF and LCD interventions to produce significant weight loss while improving body composition in patients with cirrhosis and obesity. Further research is needed to validate these findings in larger cohorts and to assess changes in muscle quality and visceral fat.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
