Jihyun Park, Chieko Kimata, Justin Young, James C Perry, Andras Bratincsak
{"title":"Fine Tuning ECG Interpretation for Young Athletes: ECG Screening Using Z-score-based Analysis.","authors":"Jihyun Park, Chieko Kimata, Justin Young, James C Perry, Andras Bratincsak","doi":"10.1186/s40798-024-00775-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Electrocardiograms (ECGs) in athletes commonly reveal findings related to physiologic adaptations to exercise, that may be difficult to discern from true underlying cardiovascular abnormalities. North American and European societies have published consensus statements for normal, borderline, and abnormal ECG findings for athletes, but these criteria are not based on established correlation with disease states. Additionally, data comparing ECG findings in athletes to non-athlete control subjects are lacking. Our objective was to compare the ECGs of collegiate athletes and non-athlete controls using Z-scores for digital ECG variables to better identify significant differences between the groups and to evaluate the ECG variables in athletes falling outside the normal range.</p><p><strong>Methods: </strong>Values for 102 digital ECG variables on 7206 subjects aged 17-22 years, including 672 athletes, from Hawaii Pacific Health, University of Hawaii, and Rady Children's Hospital San Diego were obtained through retrospective review. Age and sex-specific Z-scores for ECG variables were derived from normal subjects and used to assess the range of values for specific ECG variables in young athletes. Athletes with abnormal ECGs were referred to cardiology consultation and/or echocardiogram.</p><p><strong>Results: </strong>Athletes had slower heart rate, longer PR interval, more rightward QRS axis, longer QRS duration but shorter QTc duration, larger amplitude and area of T waves, prevalent R' waves in V1, and higher values of variables traditionally associated with left ventricular hypertrophy (LVH): amplitudes of S waves (leads V1-V2), Q waves (V6, III) and R waves (II, V5, V6). Z-scores of these ECG variables in 558 (83%) of the athletes fell within - 2.5 and 2.5 range derived from the normal population dataset, and 60 (8.9%) athletes had a Z-score outside the - 3 to 3 range. While 191 (28.4%) athletes met traditional voltage criteria for diagnosis of LVH on ECG, only 53 athletes (7.9%) had Z-scores outside the range of -2.5 to 2.5 for both S amplitude in leads V1-V2 and R amplitude in leads V5-6. Only one athlete was diagnosed with hypertrophic cardiomyopathy with a Z-score of R wave in V6 of 2.34 and T wave in V6 of -5.94.</p><p><strong>Conclusion: </strong>The use of Z-scores derived from a normal population may provide more precise screening to define cardiac abnormalities in young athletes and reduce unnecessary secondary testing, restrictions and concern.</p>","PeriodicalId":21788,"journal":{"name":"Sports Medicine - Open","volume":"10 1","pages":"114"},"PeriodicalIF":5.9000,"publicationDate":"2024-10-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11499507/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Sports Medicine - Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40798-024-00775-9","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SPORT SCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Electrocardiograms (ECGs) in athletes commonly reveal findings related to physiologic adaptations to exercise, that may be difficult to discern from true underlying cardiovascular abnormalities. North American and European societies have published consensus statements for normal, borderline, and abnormal ECG findings for athletes, but these criteria are not based on established correlation with disease states. Additionally, data comparing ECG findings in athletes to non-athlete control subjects are lacking. Our objective was to compare the ECGs of collegiate athletes and non-athlete controls using Z-scores for digital ECG variables to better identify significant differences between the groups and to evaluate the ECG variables in athletes falling outside the normal range.
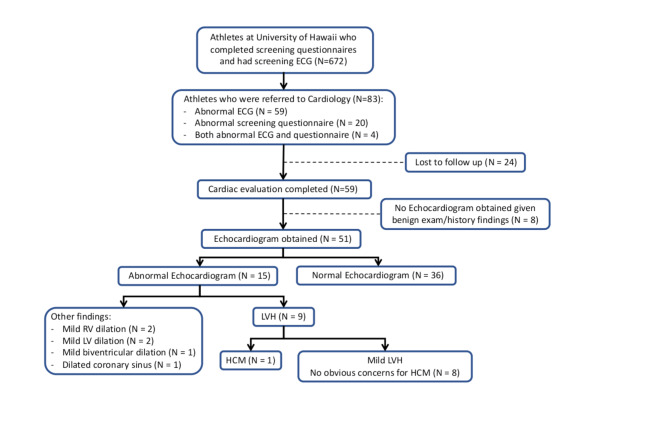
Methods: Values for 102 digital ECG variables on 7206 subjects aged 17-22 years, including 672 athletes, from Hawaii Pacific Health, University of Hawaii, and Rady Children's Hospital San Diego were obtained through retrospective review. Age and sex-specific Z-scores for ECG variables were derived from normal subjects and used to assess the range of values for specific ECG variables in young athletes. Athletes with abnormal ECGs were referred to cardiology consultation and/or echocardiogram.
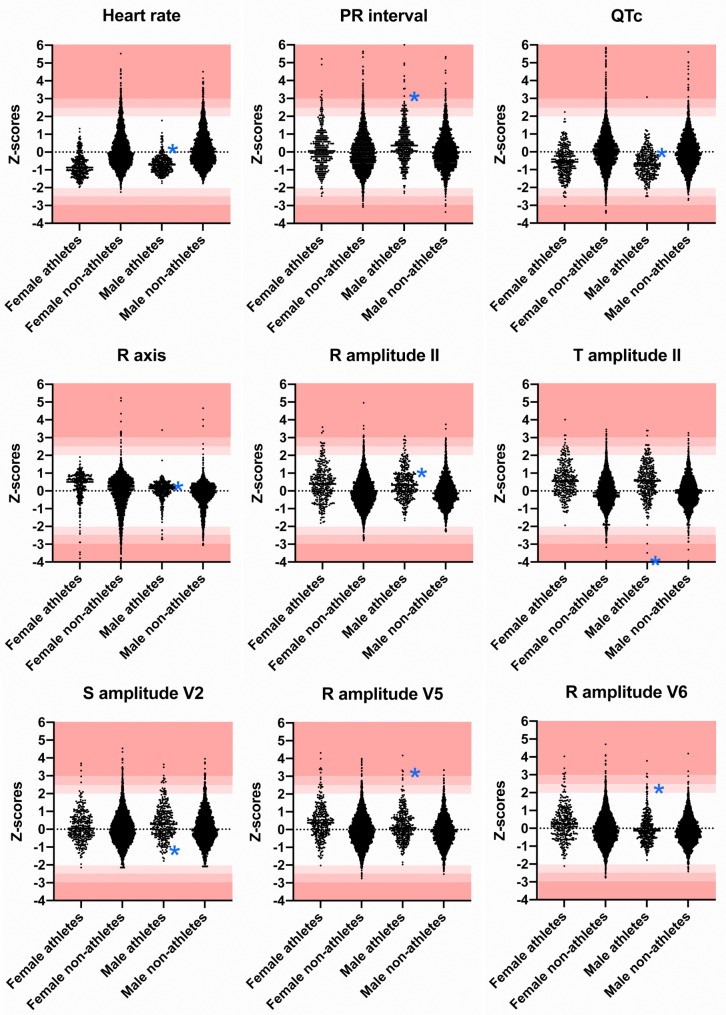
Results: Athletes had slower heart rate, longer PR interval, more rightward QRS axis, longer QRS duration but shorter QTc duration, larger amplitude and area of T waves, prevalent R' waves in V1, and higher values of variables traditionally associated with left ventricular hypertrophy (LVH): amplitudes of S waves (leads V1-V2), Q waves (V6, III) and R waves (II, V5, V6). Z-scores of these ECG variables in 558 (83%) of the athletes fell within - 2.5 and 2.5 range derived from the normal population dataset, and 60 (8.9%) athletes had a Z-score outside the - 3 to 3 range. While 191 (28.4%) athletes met traditional voltage criteria for diagnosis of LVH on ECG, only 53 athletes (7.9%) had Z-scores outside the range of -2.5 to 2.5 for both S amplitude in leads V1-V2 and R amplitude in leads V5-6. Only one athlete was diagnosed with hypertrophic cardiomyopathy with a Z-score of R wave in V6 of 2.34 and T wave in V6 of -5.94.
Conclusion: The use of Z-scores derived from a normal population may provide more precise screening to define cardiac abnormalities in young athletes and reduce unnecessary secondary testing, restrictions and concern.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
