{"title":"Growth plate closure and therapeutic interventions.","authors":"Ja Hyang Cho, Hae Woon Jung, Kye Shik Shim","doi":"10.3345/cep.2023.00346","DOIUrl":null,"url":null,"abstract":"<p><p>Height gains result from longitudinal bone growth, which is largely dependent on chondrocyte differentiation and proliferation within the growth plates of long bones. The growth plate, that is, the epiphyseal plate, is divided into resting, proliferative, and hypertrophic zones according to chondrocyte characteristics. The differentiation potential of progenitor cells in the resting zone, continuous capacity for chondrocyte differentiation and proliferation within the proliferative zone, timely replacement by osteocytes, and calcification in the hypertrophic zone are the 3 main factors controlling longitudinal bone growth. Upon adequate longitudinal bone growth, growth plate senescence limits human body height. During growth plate senescence, progenitor cells within the resting zone are depleted, proliferative chondrocyte numbers decrease, and hypertrophic chondrocyte number and size decrease. After senescence, hypertrophic chondrocytes are replaced by osteocytes, the extracellular matrix is calcified and vascularized, the growth plate is closed, and longitudinal bone growth is complete. To date, gonadotropin-releasing hormone analogs, aromatase inhibitors, C-type natriuretic peptide analogs, and fibroblast growth factor receptor 3 inhibitors have been studied or used as therapeutic interventions to delay growth plate closure. Complex networks of cellular, genetic, paracrine, and endocrine signals are involved in growth plate closure. However, the detailed mechanisms of this process remain unclear. Further elucidation of these mechanisms will enable the development of new therapeutic modalities for the treatment of short stature, precocious puberty, and skeletal dysplasia.</p>","PeriodicalId":36018,"journal":{"name":"Clinical and Experimental Pediatrics","volume":" ","pages":"553-559"},"PeriodicalIF":3.6000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11551597/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Pediatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3345/cep.2023.00346","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/28 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
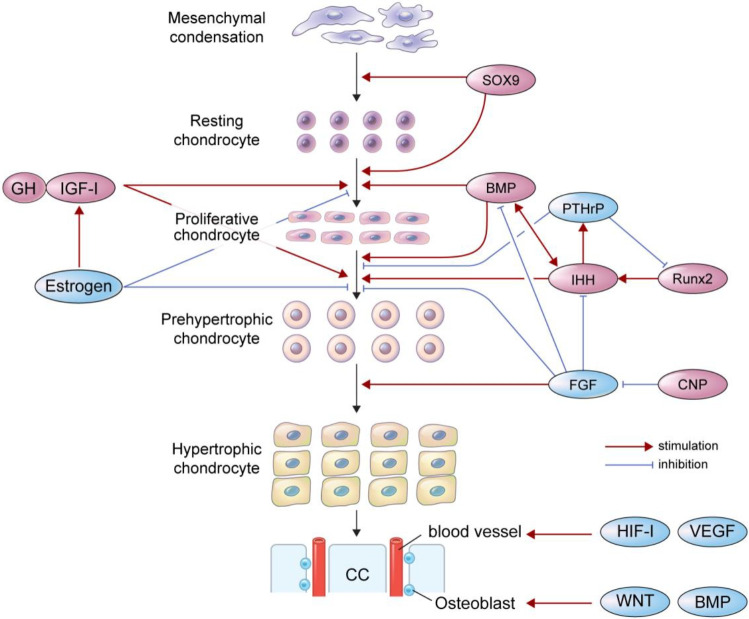
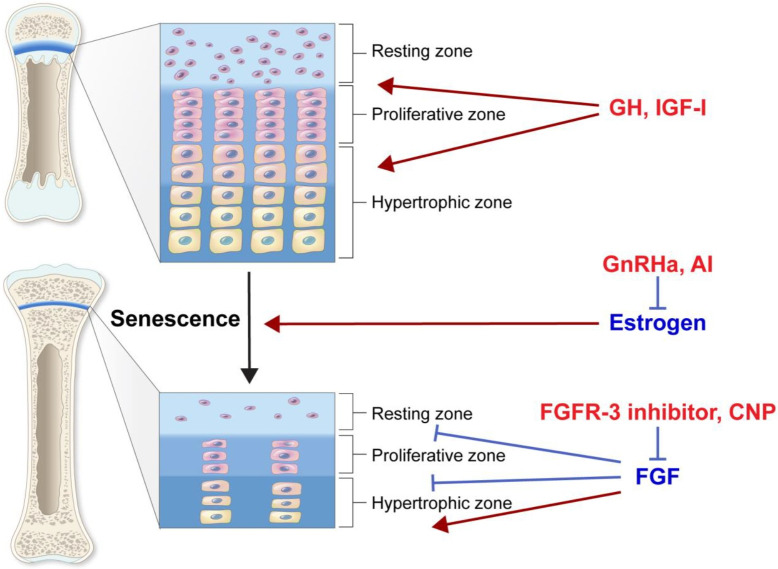
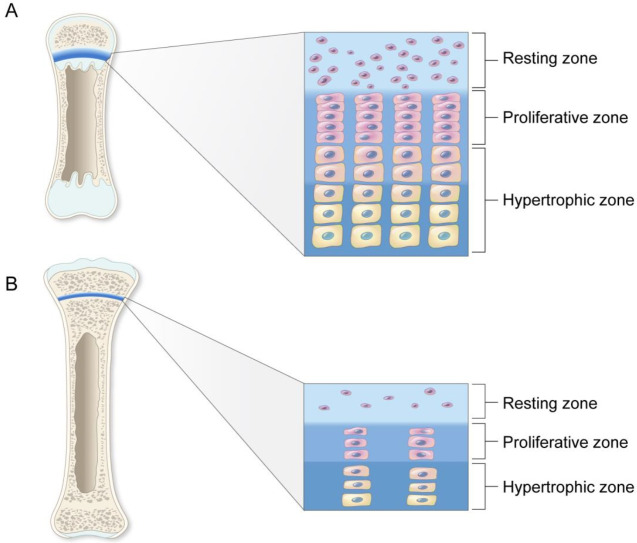
Height gains result from longitudinal bone growth, which is largely dependent on chondrocyte differentiation and proliferation within the growth plates of long bones. The growth plate, that is, the epiphyseal plate, is divided into resting, proliferative, and hypertrophic zones according to chondrocyte characteristics. The differentiation potential of progenitor cells in the resting zone, continuous capacity for chondrocyte differentiation and proliferation within the proliferative zone, timely replacement by osteocytes, and calcification in the hypertrophic zone are the 3 main factors controlling longitudinal bone growth. Upon adequate longitudinal bone growth, growth plate senescence limits human body height. During growth plate senescence, progenitor cells within the resting zone are depleted, proliferative chondrocyte numbers decrease, and hypertrophic chondrocyte number and size decrease. After senescence, hypertrophic chondrocytes are replaced by osteocytes, the extracellular matrix is calcified and vascularized, the growth plate is closed, and longitudinal bone growth is complete. To date, gonadotropin-releasing hormone analogs, aromatase inhibitors, C-type natriuretic peptide analogs, and fibroblast growth factor receptor 3 inhibitors have been studied or used as therapeutic interventions to delay growth plate closure. Complex networks of cellular, genetic, paracrine, and endocrine signals are involved in growth plate closure. However, the detailed mechanisms of this process remain unclear. Further elucidation of these mechanisms will enable the development of new therapeutic modalities for the treatment of short stature, precocious puberty, and skeletal dysplasia.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
