Karilynn M. Rockhill PhD, Gabrielle E. Bau MS, Angela DeVeaugh-Geiss PhD, Howard Chilcoat ScD, Richard Dart MD, PhD, Janetta Iwanicki MD, Joshua C. Black PhD
{"title":"Buprenorphine, oxycodone, hydrocodone, and methadone mortality in the United States (2010‒2017)","authors":"Karilynn M. Rockhill PhD, Gabrielle E. Bau MS, Angela DeVeaugh-Geiss PhD, Howard Chilcoat ScD, Richard Dart MD, PhD, Janetta Iwanicki MD, Joshua C. Black PhD","doi":"10.1002/emp2.13338","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objective</h3>\n \n <p>Opioid overdose survivors present to emergency departments (EDs) and many EDs have developed programs to initiate buprenorphine. The impact of the increasing use of buprenorphine in ED and by other providers is unknown while opioid mortality continues to rise. Public mortality data do not distinguish buprenorphine from other prescription opioids. Our objective was to determine when changes in overdose mortality trends occurred comparing deaths involving buprenorphine to oxycodone, hydrocodone, and methadone.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This observational study utilized the drug-involved mortality database including US death certificates (2010‒2017) in which buprenorphine, oxycodone, hydrocodone, or methadone were contributing causes of death (determined through textual analysis). Population- and drug utilization-adjusted mortality rates were examined using disjointed linear regression. Buprenorphine-involved deaths were stratified by polysubstance involvement.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The population-adjusted mortality rates for buprenorphine-involved deaths were lowest compared to other opioids; however, the change in rate for buprenorphine increased faster than oxycodone, hydrocodone, and methadone at 8.9% each quarter-year (95% confidence interval [CI]: 8.0, 9.8) from 2010 to mid-2016 when it stabilized. After adjusting for changes in dispensing over the study period, buprenorphine-involved mortality rates were increasing at 5.3% (95% CI: 4.6, 6.1) each quarter-year. In 2017, 94% buprenorphine-involved deaths had at least one other drug contributing to the cause of death.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Given the low mortality, high proportions of polysubstance mortality, and the mixed agonist/antagonist mechanism of action, use of buprenorphine alone likely presents a lower risk for overdose than comparators. Mortality rose faster than dispensing, signaling need to ensure people understand buprenorphine risks, particularly polysubstance use, balanced against importance for treating opioid use disorders.</p>\n </section>\n </div>","PeriodicalId":73967,"journal":{"name":"Journal of the American College of Emergency Physicians open","volume":"5 5","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-10-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11499299/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Emergency Physicians open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13338","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
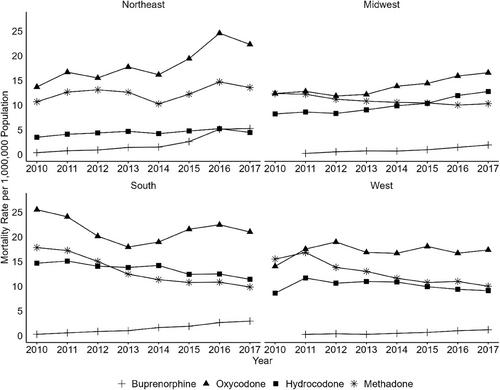
Opioid overdose survivors present to emergency departments (EDs) and many EDs have developed programs to initiate buprenorphine. The impact of the increasing use of buprenorphine in ED and by other providers is unknown while opioid mortality continues to rise. Public mortality data do not distinguish buprenorphine from other prescription opioids. Our objective was to determine when changes in overdose mortality trends occurred comparing deaths involving buprenorphine to oxycodone, hydrocodone, and methadone.
Methods
This observational study utilized the drug-involved mortality database including US death certificates (2010‒2017) in which buprenorphine, oxycodone, hydrocodone, or methadone were contributing causes of death (determined through textual analysis). Population- and drug utilization-adjusted mortality rates were examined using disjointed linear regression. Buprenorphine-involved deaths were stratified by polysubstance involvement.
Results
The population-adjusted mortality rates for buprenorphine-involved deaths were lowest compared to other opioids; however, the change in rate for buprenorphine increased faster than oxycodone, hydrocodone, and methadone at 8.9% each quarter-year (95% confidence interval [CI]: 8.0, 9.8) from 2010 to mid-2016 when it stabilized. After adjusting for changes in dispensing over the study period, buprenorphine-involved mortality rates were increasing at 5.3% (95% CI: 4.6, 6.1) each quarter-year. In 2017, 94% buprenorphine-involved deaths had at least one other drug contributing to the cause of death.
Conclusions
Given the low mortality, high proportions of polysubstance mortality, and the mixed agonist/antagonist mechanism of action, use of buprenorphine alone likely presents a lower risk for overdose than comparators. Mortality rose faster than dispensing, signaling need to ensure people understand buprenorphine risks, particularly polysubstance use, balanced against importance for treating opioid use disorders.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
