Comparison of Two Methods of Antepartum Anticoagulation: Continuation of Enoxaparin until Scheduled Induction of Labor Versus Transitioning to Heparin with Spontaneous Labor.
Marcia DesJardin, Edward Raff, Brian James, Angelina Mozier, Nicholas Baranco, Dimitrios Mastrogiannis
{"title":"Comparison of Two Methods of Antepartum Anticoagulation: Continuation of Enoxaparin until Scheduled Induction of Labor Versus Transitioning to Heparin with Spontaneous Labor.","authors":"Marcia DesJardin, Edward Raff, Brian James, Angelina Mozier, Nicholas Baranco, Dimitrios Mastrogiannis","doi":"10.1089/whr.2024.0039","DOIUrl":null,"url":null,"abstract":"<p><p>Pregnancy is a hypercoagulable state. There is a lack of strong evidence-based guidance regarding management when anticoagulation is required to prevent or treat venous thromboembolism during pregnancy. In practice, some patients are prescribed enoxaparin and transitioned to heparin due to the shorter half-life in the setting of an unpredictable delivery despite less predictable pharmacokinetics of heparin compared with enoxaparin, while others are continued on enoxaparin with a scheduled delivery. This work retrospectively evaluates obstetrical and neonatal outcomes between these two practices for 194 live singleton deliveries from 179 patients in a single institution January 2017 through May 2022. A Bayesian regression was used to control for confounders including dosing regimens. This work found no statistically significant differences in blood loss at time of delivery or availability of neuraxial anesthesia. This suggests continuing enoxaparin is noninferior to transitioning to heparin when anticoagulation is indicated in pregnancy.</p>","PeriodicalId":75329,"journal":{"name":"Women's health reports (New Rochelle, N.Y.)","volume":"5 1","pages":"720-726"},"PeriodicalIF":1.8000,"publicationDate":"2024-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11512085/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Women's health reports (New Rochelle, N.Y.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/whr.2024.0039","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
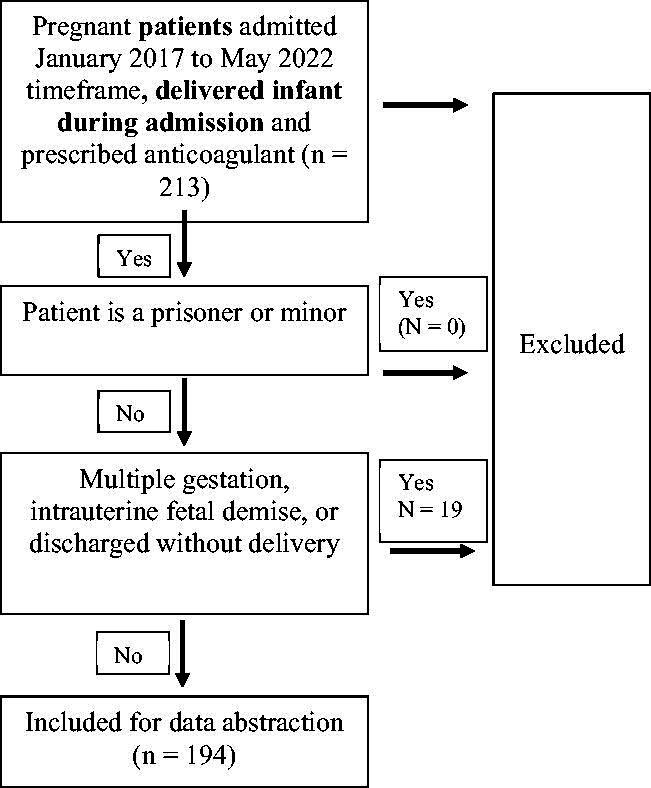
Pregnancy is a hypercoagulable state. There is a lack of strong evidence-based guidance regarding management when anticoagulation is required to prevent or treat venous thromboembolism during pregnancy. In practice, some patients are prescribed enoxaparin and transitioned to heparin due to the shorter half-life in the setting of an unpredictable delivery despite less predictable pharmacokinetics of heparin compared with enoxaparin, while others are continued on enoxaparin with a scheduled delivery. This work retrospectively evaluates obstetrical and neonatal outcomes between these two practices for 194 live singleton deliveries from 179 patients in a single institution January 2017 through May 2022. A Bayesian regression was used to control for confounders including dosing regimens. This work found no statistically significant differences in blood loss at time of delivery or availability of neuraxial anesthesia. This suggests continuing enoxaparin is noninferior to transitioning to heparin when anticoagulation is indicated in pregnancy.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
