{"title":"Predicting Sepsis-Related Mortality: Pitt Bacteremia Score is Superior to the Charlson Comorbidity Index","authors":"Şenay Öztürk Durmaz, Ayşenur Sümer Coşkun","doi":"10.1155/2024/6996399","DOIUrl":null,"url":null,"abstract":"<div>\n <p><b>Aim:</b> To assess the role of Pitt bacteremia score (PBS) and Charlson Comorbidity Index (CCI) in predicting mortality among patients with intensive care unit (ICU)–acquired Gram-negative bacterial sepsis and to investigate other factors associated with mortality.</p>\n <p><b>Methods:</b> This retrospective study was carried out between January 2018 and January 2023. Patients diagnosed with ICU-acquired sepsis caused by Gram-negative bacteria were included in the study. Demographics, laboratory data, blood culture results, management, length of ICU stay, mortality, and other clinical data were recorded. PBS and CCI score were calculated based on data collected at time of blood withdrawal. The primary endpoint was mortality in ICU.</p>\n <p><b>Results:</b> Among the 425 patients included in the study, mortality was observed in 268 (63%). Age and sex were distributed similarly in the mortality and survival groups. CCI score with a cutoff value of > 5.5 (AUC = 0.611) and PBS with a cutoff value of > 2.5 (AUC = 0.904) were able to significantly predict mortality. Multivariable logistic regression revealed that mortality was independently associated with having any comorbidity, congestive heart failure, low platelet count, high lactate, high (> 2.5) PBS, and carbapenem resistance (<i>p</i> = 0.001).</p>\n <p><b>Conclusion:</b> PBS was more successful than CCI in predicting mortality in patients with ICU-acquired sepsis caused by Gram-negative bacteria. In addition to higher PBS, having any comorbidity (and additionally, congestive heart failure), lower platelet, higher lactate, and carbapenem resistance were risk factors for mortality.</p>\n </div>","PeriodicalId":13782,"journal":{"name":"International Journal of Clinical Practice","volume":"2024 1","pages":""},"PeriodicalIF":2.4000,"publicationDate":"2024-10-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/6996399","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Clinical Practice","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1155/2024/6996399","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: To assess the role of Pitt bacteremia score (PBS) and Charlson Comorbidity Index (CCI) in predicting mortality among patients with intensive care unit (ICU)–acquired Gram-negative bacterial sepsis and to investigate other factors associated with mortality.
Methods: This retrospective study was carried out between January 2018 and January 2023. Patients diagnosed with ICU-acquired sepsis caused by Gram-negative bacteria were included in the study. Demographics, laboratory data, blood culture results, management, length of ICU stay, mortality, and other clinical data were recorded. PBS and CCI score were calculated based on data collected at time of blood withdrawal. The primary endpoint was mortality in ICU.
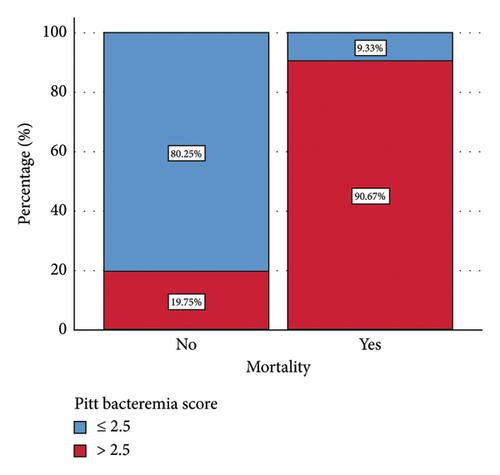
Results: Among the 425 patients included in the study, mortality was observed in 268 (63%). Age and sex were distributed similarly in the mortality and survival groups. CCI score with a cutoff value of > 5.5 (AUC = 0.611) and PBS with a cutoff value of > 2.5 (AUC = 0.904) were able to significantly predict mortality. Multivariable logistic regression revealed that mortality was independently associated with having any comorbidity, congestive heart failure, low platelet count, high lactate, high (> 2.5) PBS, and carbapenem resistance (p = 0.001).
Conclusion: PBS was more successful than CCI in predicting mortality in patients with ICU-acquired sepsis caused by Gram-negative bacteria. In addition to higher PBS, having any comorbidity (and additionally, congestive heart failure), lower platelet, higher lactate, and carbapenem resistance were risk factors for mortality.
期刊介绍:
IJCP is a general medical journal. IJCP gives special priority to work that has international appeal.
IJCP publishes:
Editorials. IJCP Editorials are commissioned. [Peer reviewed at the editor''s discretion]
Perspectives. Most IJCP Perspectives are commissioned. Example. [Peer reviewed at the editor''s discretion]
Study design and interpretation. Example. [Always peer reviewed]
Original data from clinical investigations. In particular: Primary research papers from RCTs, observational studies, epidemiological studies; pre-specified sub-analyses; pooled analyses. [Always peer reviewed]
Meta-analyses. [Always peer reviewed]
Systematic reviews. From October 2009, special priority will be given to systematic reviews. [Always peer reviewed]
Non-systematic/narrative reviews. From October 2009, reviews that are not systematic will be considered only if they include a discrete Methods section that must explicitly describe the authors'' approach. Special priority will, however, be given to systematic reviews. [Always peer reviewed]
''How to…'' papers. Example. [Always peer reviewed]
Consensus statements. [Always peer reviewed] Short reports. [Always peer reviewed]
Letters. [Peer reviewed at the editor''s discretion]
International scope
IJCP publishes work from investigators globally. Around 30% of IJCP articles list an author from the UK. Around 30% of IJCP articles list an author from the USA or Canada. Around 45% of IJCP articles list an author from a European country that is not the UK. Around 15% of articles published in IJCP list an author from a country in the Asia-Pacific region.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
