{"title":"Transileocolic Portal Vein Embolization Increases Remnant Liver Volume After Major Hepatectomy.","authors":"Koichi Kimura, Ryosuke Minagawa, Terutoshi Yamaoka, Takuma Izumi, Y U Takahashi, Mitsuru Nakanishi, Takayuki Tokunaga, Daisuke Matsuda, Yoshinari Nobuto, Hiroko Yano, Yuichiro Kajiwara, Kenichi Honma, Shigeyuki Nagata, Kazuhito Minami, Takashi Nishizaki","doi":"10.21873/invivo.13755","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aim: </strong>Transileocolic portal vein embolization (TIPE) may reduce the risk of liver failure after massive hepatectomy. However, convincing evidence of its usefulness in this regard is yet to be reported. Therefore, this study aimed to investigate the use of TIPE after massive hepatectomy.</p><p><strong>Patients and methods: </strong>Twelve patients who underwent TIPE were included. Pre- and postoperative liver volumetry was determined using a 3D simulator with computed tomography.</p><p><strong>Results: </strong>After TIPE, the percent change in total liver volume was 104.0%±13.1% (p=0.08). Conversely, the percent increase in remnant liver volume (ml)/total liver volume (ml) and remnant liver volume (ml)/standard liver volume (ml) was 122.9%±18.6% (p<0.001) and 132.2%±19.6% (p<0.001), respectively. TIPE operation time was 125±84.6 min, with minimal blood loss in all cases. Postoperative hospitalization duration during TIPE was 4.5±2.6 days. No TIPE-related complications occurred in any patient.</p><p><strong>Conclusion: </strong>TIPE is beneficial and safe when preoperative volumetry indicates that the remaining liver volume is inadequate and inoperable.</p>","PeriodicalId":13364,"journal":{"name":"In vivo","volume":"38 6","pages":"2761-2766"},"PeriodicalIF":1.8000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11535930/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"In vivo","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21873/invivo.13755","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background/aim: Transileocolic portal vein embolization (TIPE) may reduce the risk of liver failure after massive hepatectomy. However, convincing evidence of its usefulness in this regard is yet to be reported. Therefore, this study aimed to investigate the use of TIPE after massive hepatectomy.
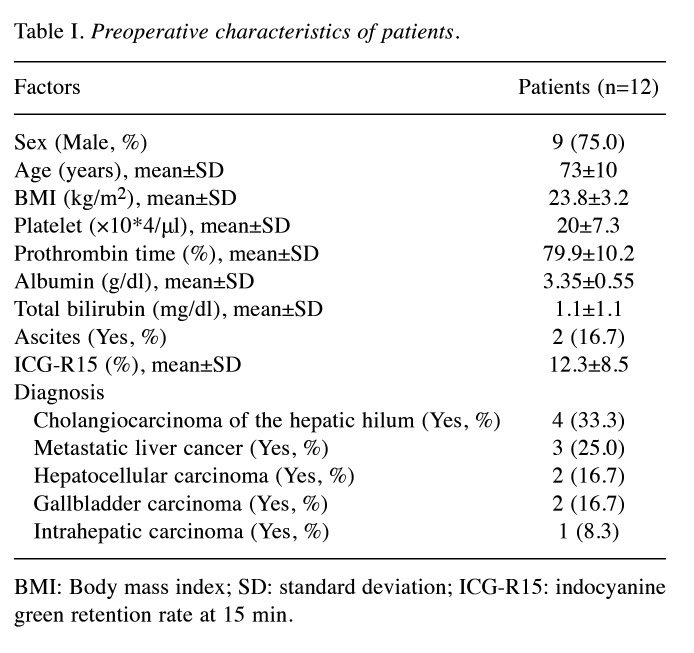
Patients and methods: Twelve patients who underwent TIPE were included. Pre- and postoperative liver volumetry was determined using a 3D simulator with computed tomography.
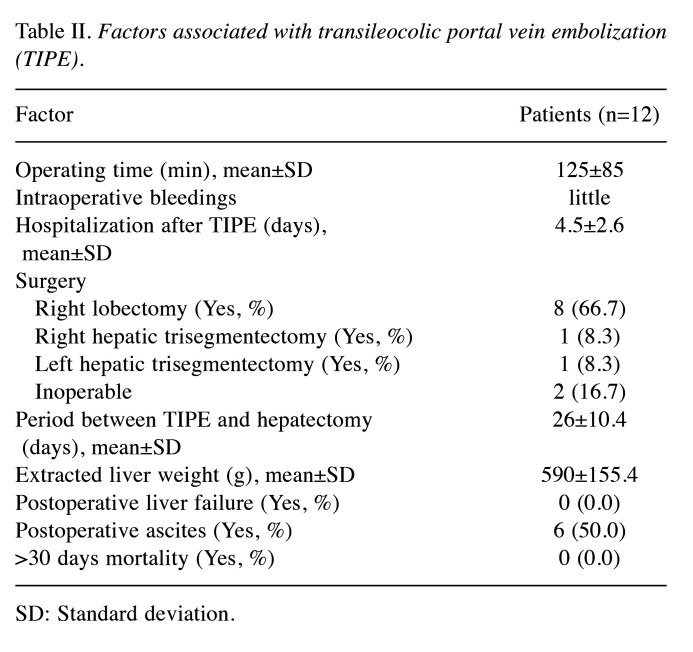
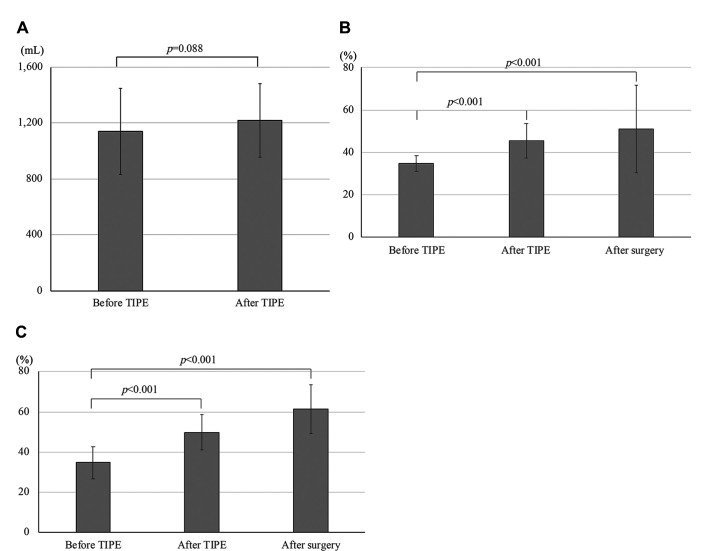
Results: After TIPE, the percent change in total liver volume was 104.0%±13.1% (p=0.08). Conversely, the percent increase in remnant liver volume (ml)/total liver volume (ml) and remnant liver volume (ml)/standard liver volume (ml) was 122.9%±18.6% (p<0.001) and 132.2%±19.6% (p<0.001), respectively. TIPE operation time was 125±84.6 min, with minimal blood loss in all cases. Postoperative hospitalization duration during TIPE was 4.5±2.6 days. No TIPE-related complications occurred in any patient.
Conclusion: TIPE is beneficial and safe when preoperative volumetry indicates that the remaining liver volume is inadequate and inoperable.
背景/目的:经结肠门静脉栓塞术(TIPE)可降低大块肝切除术后肝功能衰竭的风险。然而,目前尚未有令人信服的证据证明其在这方面的作用。因此,本研究旨在调查大面积肝切除术后 TIPE 的使用情况:纳入了 12 名接受 TIPE 的患者。结果:TIPE术后,肝脏体积变化的百分比与TIPE术后肝脏体积变化的百分比相同:结果:TIPE术后,肝脏总体积的变化率为104.0%±13.1%(P=0.08)。相反,残余肝脏体积(毫升)/肝脏总体积(毫升)和残余肝脏体积(毫升)/标准肝脏体积(毫升)的增加百分比为 122.9%±18.6%(P=0.08):当术前肝脏容积测量显示剩余肝脏容积不足且无法手术时,TIPE是有益且安全的。
期刊介绍:
IN VIVO is an international peer-reviewed journal designed to bring together original high quality works and reviews on experimental and clinical biomedical research within the frames of physiology, pathology and disease management.
The topics of IN VIVO include: 1. Experimental development and application of new diagnostic and therapeutic procedures; 2. Pharmacological and toxicological evaluation of new drugs, drug combinations and drug delivery systems; 3. Clinical trials; 4. Development and characterization of models of biomedical research; 5. Cancer diagnosis and treatment; 6. Immunotherapy and vaccines; 7. Radiotherapy, Imaging; 8. Tissue engineering, Regenerative medicine; 9. Carcinogenesis.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
