Abhishek Dattani, Jian L Yeo, Emer M Brady, Alice Cowley, Anna-Marie Marsh, Manjit Sian, Joanna M Bilak, Matthew P M Graham-Brown, Anvesha Singh, Jayanth R Arnold, David Adlam, Thomas Yates, Gerry P McCann, Gaurav S Gulsin
{"title":"Association between subclinical right ventricular alterations and aerobic exercise capacity in type 2 diabetes.","authors":"Abhishek Dattani, Jian L Yeo, Emer M Brady, Alice Cowley, Anna-Marie Marsh, Manjit Sian, Joanna M Bilak, Matthew P M Graham-Brown, Anvesha Singh, Jayanth R Arnold, David Adlam, Thomas Yates, Gerry P McCann, Gaurav S Gulsin","doi":"10.1016/j.jocmr.2024.101120","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Type 2 diabetes (T2D) leads to cardiovascular remodeling, and heart failure has emerged as a major complication of T2D. There is a limited understanding of the impact of T2D on the right heart. This study aimed to assess subclinical right heart alterations and their contribution to aerobic exercise capacity (peak oxygen consumption; peak VO<sub>2</sub>) in adults with T2D.</p><p><strong>Methods: </strong>Single center, prospective, case-control comparison of adults with and without T2D, and no prevalent cardiac disease. Comprehensive evaluation of the left and right heart was performed using transthoracic echocardiography and stress cardiovascular magnetic resonance. Cardiopulmonary exercise testing on a bicycle ergometer with expired gas analysis was performed to determine peak VO<sub>2</sub>. Between group comparison was adjusted for age, sex, race, and body mass index using analysis of covariance (ANCOVA). Multivariable linear regression, including key clinical and left heart variables, was undertaken in people with T2D to identify independent associations between measures of right ventricular (RV) structure and function with peak VO<sub>2</sub>.</p><p><strong>Results: </strong>Three hundred and forty people with T2D (median age 64years, 62% (211) male, mean glycated hemoglobin (HbA1c) 7.3%) and 66 controls (median age 58years, 58% (38) male, mean HbA1c 5.5%) were included. T2D participants had markedly lower peak VO<sub>2</sub> (adjusted mean 20.3 (95% confidence interval (CI): 19.8-20.9) vs 23.3(22.2-24.5)mL/kg/min, P < 0.001) than controls and had smaller left ventricular (LV) volumes and LV concentric remodeling. Those with T2D had smaller RV volumes (indexed RV end-diastolic volume: 84 (82-86) vs 100 (96-104)mL/m, P < 0.001) with evidence of hyperdynamic RV systolic function (global longitudinal strain (GLS): 26.3 (25.8-26.8) vs 23.5 (22.5-24.5)%, P < 0.001) and impaired RV relaxation (longitudinal peak early diastolic strain rate (PEDSR): 0.77 (0.74-0.80) vs 0.92 (0.85-1.00) s<sup>-1</sup>, P < 0.001). Multivariable linear regression demonstrated that RV end-diastolic volume (β =-0.342, P = 0.004) and RV cardiac output (β = 0.296, P = 0.001), but not LV parameters, were independent determinants of peak VO<sub>2</sub>.</p><p><strong>Conclusion: </strong>In T2D, markers of RV remodeling are associated with aerobic exercise capacity, independent of left heart alterations.</p>","PeriodicalId":15221,"journal":{"name":"Journal of Cardiovascular Magnetic Resonance","volume":" ","pages":"101120"},"PeriodicalIF":6.1000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11663768/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Magnetic Resonance","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.jocmr.2024.101120","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/28 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Type 2 diabetes (T2D) leads to cardiovascular remodeling, and heart failure has emerged as a major complication of T2D. There is a limited understanding of the impact of T2D on the right heart. This study aimed to assess subclinical right heart alterations and their contribution to aerobic exercise capacity (peak oxygen consumption; peak VO2) in adults with T2D.
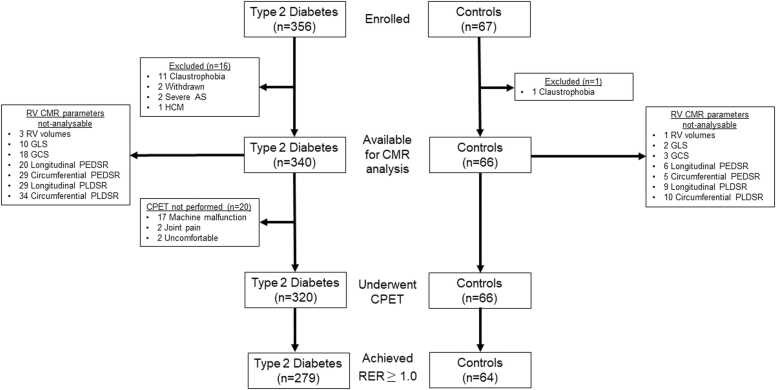
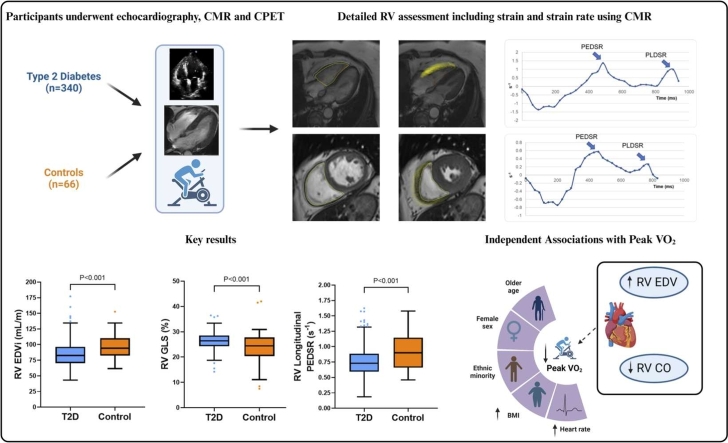
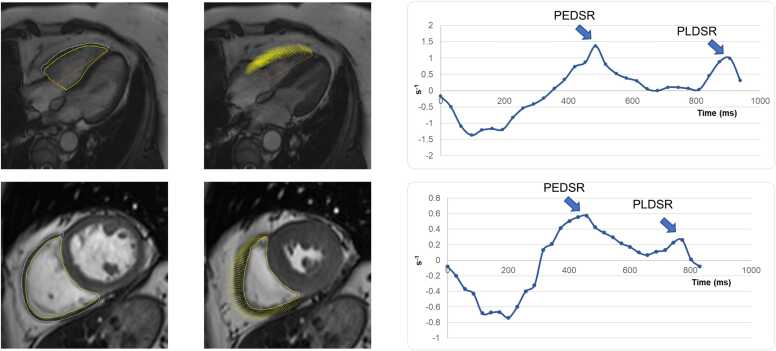
Methods: Single center, prospective, case-control comparison of adults with and without T2D, and no prevalent cardiac disease. Comprehensive evaluation of the left and right heart was performed using transthoracic echocardiography and stress cardiovascular magnetic resonance. Cardiopulmonary exercise testing on a bicycle ergometer with expired gas analysis was performed to determine peak VO2. Between group comparison was adjusted for age, sex, race, and body mass index using analysis of covariance (ANCOVA). Multivariable linear regression, including key clinical and left heart variables, was undertaken in people with T2D to identify independent associations between measures of right ventricular (RV) structure and function with peak VO2.
Results: Three hundred and forty people with T2D (median age 64years, 62% (211) male, mean glycated hemoglobin (HbA1c) 7.3%) and 66 controls (median age 58years, 58% (38) male, mean HbA1c 5.5%) were included. T2D participants had markedly lower peak VO2 (adjusted mean 20.3 (95% confidence interval (CI): 19.8-20.9) vs 23.3(22.2-24.5)mL/kg/min, P < 0.001) than controls and had smaller left ventricular (LV) volumes and LV concentric remodeling. Those with T2D had smaller RV volumes (indexed RV end-diastolic volume: 84 (82-86) vs 100 (96-104)mL/m, P < 0.001) with evidence of hyperdynamic RV systolic function (global longitudinal strain (GLS): 26.3 (25.8-26.8) vs 23.5 (22.5-24.5)%, P < 0.001) and impaired RV relaxation (longitudinal peak early diastolic strain rate (PEDSR): 0.77 (0.74-0.80) vs 0.92 (0.85-1.00) s-1, P < 0.001). Multivariable linear regression demonstrated that RV end-diastolic volume (β =-0.342, P = 0.004) and RV cardiac output (β = 0.296, P = 0.001), but not LV parameters, were independent determinants of peak VO2.
Conclusion: In T2D, markers of RV remodeling are associated with aerobic exercise capacity, independent of left heart alterations.
期刊介绍:
Journal of Cardiovascular Magnetic Resonance (JCMR) publishes high-quality articles on all aspects of basic, translational and clinical research on the design, development, manufacture, and evaluation of cardiovascular magnetic resonance (CMR) methods applied to the cardiovascular system. Topical areas include, but are not limited to:
New applications of magnetic resonance to improve the diagnostic strategies, risk stratification, characterization and management of diseases affecting the cardiovascular system.
New methods to enhance or accelerate image acquisition and data analysis.
Results of multicenter, or larger single-center studies that provide insight into the utility of CMR.
Basic biological perceptions derived by CMR methods.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
