Adherence to First-Line Intravesical Bacillus Calmette-Guérin Therapy in the Context of Guideline Recommendations for US Patients With High-Risk Non-muscle Invasive Bladder Cancer.
Franklin D Gaylis, Bruno Emond, Ameur M Manceur, Anabelle Tardif-Samson, Laura Morrison, Dominic Pilon, Patrick Lefebvre, Lorie A Ellis, Hiremagalur Balaji, Andrea Ireland
{"title":"Adherence to First-Line Intravesical Bacillus Calmette-Guérin Therapy in the Context of Guideline Recommendations for US Patients With High-Risk Non-muscle Invasive Bladder Cancer.","authors":"Franklin D Gaylis, Bruno Emond, Ameur M Manceur, Anabelle Tardif-Samson, Laura Morrison, Dominic Pilon, Patrick Lefebvre, Lorie A Ellis, Hiremagalur Balaji, Andrea Ireland","doi":"10.36469/001c.124208","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Bacillus Calmette-Guérin (BCG) can reduce recurrence and delay progression among patients with high-risk non-muscle invasive bladder cancer (NMIBC), but is associated with a substantial emotional, physical, and social burden. <b>Objectives:</b> This study evaluated the adequacy of first-line intravesical BCG treatment among high-risk NMIBC patients in the United States, including the subgroup with carcinoma in situ (CIS) of the bladder. <b>Methods:</b> Adults with high-risk NMIBC treated with BCG were selected from de-identified MarketScan® Commercial, Medicare, and Medicaid Databases (1/1/2010-2/28/2021). Adequacy of BCG induction and maintenance was evaluated from the first BCG claim until the end of the patient's observation, using a previously published claims-based algorithm (induction: ≥5 instillations within 70 days; induction and maintenance: ≥7 instillations within 274 days of first instillation) and a definition based on the landmark Southwest Oncology Group (SWOG) trial (induction: ≥5 instillations without gaps >7 days; followed by ≥2 instillations at month 3, 6, and every 6 months thereafter). Proportions of patients with adequate BCG induction and maintenance were reported overall and compared between those with and without CIS. <b>Results:</b> Of 5803 high-risk NMIBC patients treated with first-line BCG (mean age, 67.3 years; 20.6% female), 930 (16.0%) had CIS. After first-line BCG, 56.6% received another treatment. Although 86.9% had adequate BCG induction based on the claims-based algorithm (SWOG, 73.6%), only 41.5% had adequate BCG induction and maintenance (SWOG, 1.6%). Similar trends were observed for patients with and without CIS, with higher adherence to guidelines for patients with CIS (adequate induction using claims-based algorithm: 90.3% vs 86.2%; adequate induction and maintenance: 50.8% vs 39.7%, all <i>P</i> < .001). A greater proportion of CIS patients than non-CIS patients had cystectomy (CIS, 14.4%, non-CIS, 8.5%; <i>P</i> < .001) after first-line BCG. <b>Discussion:</b> Among patients with NMIBC treated with first-line intravesical BCG, most received adequate BCG induction but less than half had adequate BCG maintenance. BCG treatment was also inadequate for patients with CIS, with only half of patients receiving adequate BCG maintenance and a higher proportion undergoing cystectomy following first-line BCG. <b>Conclusions:</b> Results emphasize the need for additional treatment options for patients with NMIBC.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"11 2","pages":"109-117"},"PeriodicalIF":2.3000,"publicationDate":"2024-10-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11523569/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.124208","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
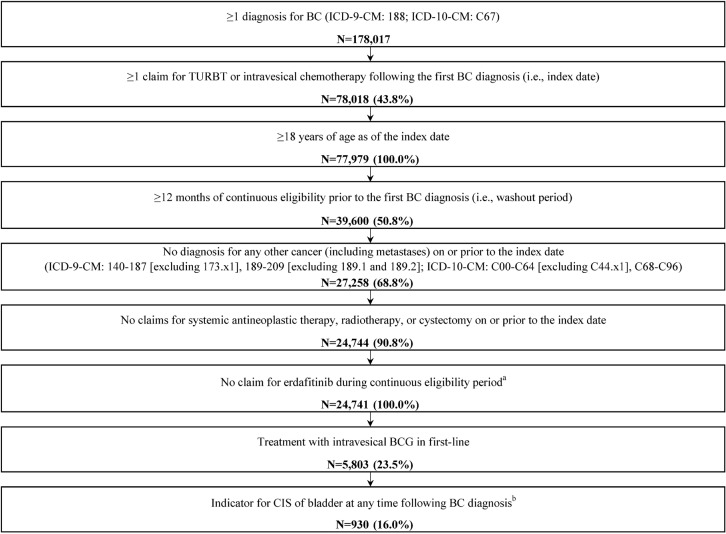
Background: Bacillus Calmette-Guérin (BCG) can reduce recurrence and delay progression among patients with high-risk non-muscle invasive bladder cancer (NMIBC), but is associated with a substantial emotional, physical, and social burden. Objectives: This study evaluated the adequacy of first-line intravesical BCG treatment among high-risk NMIBC patients in the United States, including the subgroup with carcinoma in situ (CIS) of the bladder. Methods: Adults with high-risk NMIBC treated with BCG were selected from de-identified MarketScan® Commercial, Medicare, and Medicaid Databases (1/1/2010-2/28/2021). Adequacy of BCG induction and maintenance was evaluated from the first BCG claim until the end of the patient's observation, using a previously published claims-based algorithm (induction: ≥5 instillations within 70 days; induction and maintenance: ≥7 instillations within 274 days of first instillation) and a definition based on the landmark Southwest Oncology Group (SWOG) trial (induction: ≥5 instillations without gaps >7 days; followed by ≥2 instillations at month 3, 6, and every 6 months thereafter). Proportions of patients with adequate BCG induction and maintenance were reported overall and compared between those with and without CIS. Results: Of 5803 high-risk NMIBC patients treated with first-line BCG (mean age, 67.3 years; 20.6% female), 930 (16.0%) had CIS. After first-line BCG, 56.6% received another treatment. Although 86.9% had adequate BCG induction based on the claims-based algorithm (SWOG, 73.6%), only 41.5% had adequate BCG induction and maintenance (SWOG, 1.6%). Similar trends were observed for patients with and without CIS, with higher adherence to guidelines for patients with CIS (adequate induction using claims-based algorithm: 90.3% vs 86.2%; adequate induction and maintenance: 50.8% vs 39.7%, all P < .001). A greater proportion of CIS patients than non-CIS patients had cystectomy (CIS, 14.4%, non-CIS, 8.5%; P < .001) after first-line BCG. Discussion: Among patients with NMIBC treated with first-line intravesical BCG, most received adequate BCG induction but less than half had adequate BCG maintenance. BCG treatment was also inadequate for patients with CIS, with only half of patients receiving adequate BCG maintenance and a higher proportion undergoing cystectomy following first-line BCG. Conclusions: Results emphasize the need for additional treatment options for patients with NMIBC.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
