{"title":"Circulatory characteristics of early mobilization after surgery for bilateral pheochromocytoma: a case report.","authors":"Kenichi Fudeyasu, Satoshi Kamiya, Shunsuke Taito, Yuki Nakashima, Makoto Asaeda, Takahiro Kato, Yukari Toyota, Hiroyuki Kitano, Nobuyuki Hinata, Haruya Ohno, Yukio Mikami","doi":"10.1186/s13256-024-04833-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Surgical treatment of pheochromocytomas is associated with circulatory dynamics instability, necessitating systemic management of the patient in the intensive care unit after surgery. Early mobilization after pheochromocytoma surgery is not described in the guidelines, and to our knowledge, no reports have specifically focused on circulatory dynamics during early mobilization after surgery.</p><p><strong>Case presentation: </strong>A 31-year-old Japanese woman was diagnosed with bilateral pheochromocytoma and underwent a second-stage adrenalectomy for bilateral pheochromocytoma at our hospital. We evaluated circulatory dynamics during a passive upright posture on postoperative days 1 and 4. She was placed on a tilt bed in the supine position (0° head) for 15 min, passive upright posture (60°) for 15 min, and supine position again for 10 min. In the passive upright posture, both systolic and diastolic blood pressure decreased, and the heart rate increased by 10 bpm over approximately 10 minutes. After the postural change from the passive upright posture to the supine position, the heart rate decreased to a level lower than in the supine prior to the passive upright posture. The same measurements were taken on postoperative day 4. Systolic blood pressure decreased in the passive upright posture, but diastolic blood pressure remained unchanged. The heart rate also increased earlier after passive upright posture compared with that on the day after surgery. When the patient returned to the supine position from the passive upright posture, the heart rate decreased even further compared with its level prior to the passive upright posture, as observed on the day after surgery.</p><p><strong>Conclusion: </strong>Circulatory dynamics may fluctuate after surgery for pheochromocytoma due to a relative decrease in epinephrine and norepinephrine secretion. In this case, the patient's response may be close to normal by the fourth postoperative day, but circulatory dynamics fluctuations were noted on both the first and fourth postoperative days when the patient was supine after passive upright posture. Although the substantial variability of perioperative circulatory dynamics in patients with pheochromocytoma has improved considerably with the development of perioperative management guidelines, circulatory dynamics should be carefully monitored during early mobilization and after its completion.</p>","PeriodicalId":16236,"journal":{"name":"Journal of Medical Case Reports","volume":"18 1","pages":"529"},"PeriodicalIF":0.8000,"publicationDate":"2024-10-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11526685/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13256-024-04833-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Surgical treatment of pheochromocytomas is associated with circulatory dynamics instability, necessitating systemic management of the patient in the intensive care unit after surgery. Early mobilization after pheochromocytoma surgery is not described in the guidelines, and to our knowledge, no reports have specifically focused on circulatory dynamics during early mobilization after surgery.
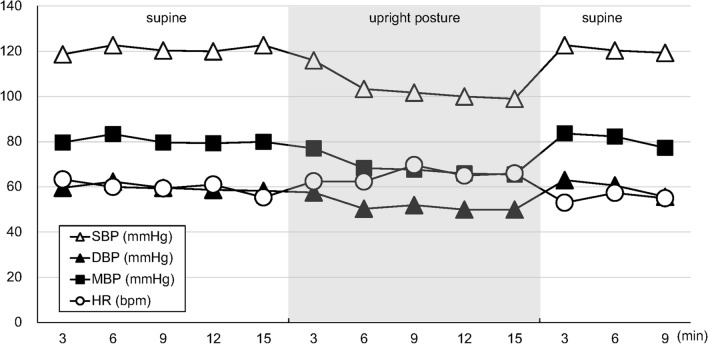
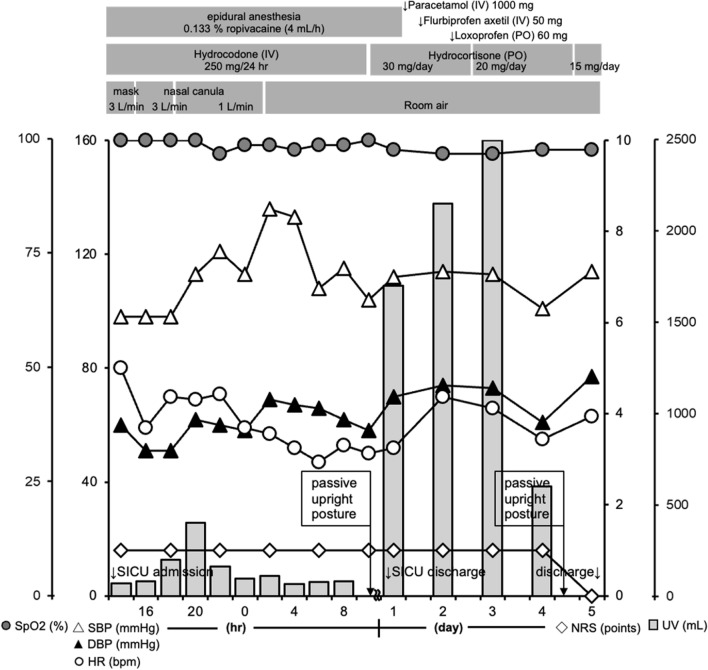
Case presentation: A 31-year-old Japanese woman was diagnosed with bilateral pheochromocytoma and underwent a second-stage adrenalectomy for bilateral pheochromocytoma at our hospital. We evaluated circulatory dynamics during a passive upright posture on postoperative days 1 and 4. She was placed on a tilt bed in the supine position (0° head) for 15 min, passive upright posture (60°) for 15 min, and supine position again for 10 min. In the passive upright posture, both systolic and diastolic blood pressure decreased, and the heart rate increased by 10 bpm over approximately 10 minutes. After the postural change from the passive upright posture to the supine position, the heart rate decreased to a level lower than in the supine prior to the passive upright posture. The same measurements were taken on postoperative day 4. Systolic blood pressure decreased in the passive upright posture, but diastolic blood pressure remained unchanged. The heart rate also increased earlier after passive upright posture compared with that on the day after surgery. When the patient returned to the supine position from the passive upright posture, the heart rate decreased even further compared with its level prior to the passive upright posture, as observed on the day after surgery.
Conclusion: Circulatory dynamics may fluctuate after surgery for pheochromocytoma due to a relative decrease in epinephrine and norepinephrine secretion. In this case, the patient's response may be close to normal by the fourth postoperative day, but circulatory dynamics fluctuations were noted on both the first and fourth postoperative days when the patient was supine after passive upright posture. Although the substantial variability of perioperative circulatory dynamics in patients with pheochromocytoma has improved considerably with the development of perioperative management guidelines, circulatory dynamics should be carefully monitored during early mobilization and after its completion.
期刊介绍:
JMCR is an open access, peer-reviewed online journal that will consider any original case report that expands the field of general medical knowledge. Reports should show one of the following: 1. Unreported or unusual side effects or adverse interactions involving medications 2. Unexpected or unusual presentations of a disease 3. New associations or variations in disease processes 4. Presentations, diagnoses and/or management of new and emerging diseases 5. An unexpected association between diseases or symptoms 6. An unexpected event in the course of observing or treating a patient 7. Findings that shed new light on the possible pathogenesis of a disease or an adverse effect




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
