{"title":"Atraumatic Splenic Rupture Unveiling Mumps With an Underlying B-cell Lymphoid Hyperplasia: A Diagnostic Conundrum.","authors":"Inderjeet Singh, Hariharasudhan Balaji, Nithin Jyothy","doi":"10.7759/cureus.72671","DOIUrl":null,"url":null,"abstract":"<p><p>Atraumatic splenic rupture (ASR) is an unfamiliar entity that is potentially life-threatening if there is a delay in the diagnosis. Due to its rarity and its non-specific presentation, it can be a challenge to diagnose early. In this report, we present a case of a 42-year-old male patient who presented to the emergency department with nonspecific abdominal pain and had no past medical history. The patient presented abdominal pain associated with nausea, vomiting, and sweating. On examination, the patient was found to be tachycardic and mildly hypotensive, with mild left upper quadrant tenderness, and a lactate of 4 mmol/L on venous blood gas analysis. He was urgently transferred to the resuscitation area, where resuscitation commenced. Further investigations revealed significant anemia. The contrast-enhanced CT of the abdomen performed revealed a 13-cm splenic hemostasis suggestive of non-traumatic splenic rupture. The patient lacked any history of blunt trauma or family history that could account for the splenic rupture. The patient was taken to the theatre by the surgical team as he remained unstable. He received four units of blood in the theatre and underwent splenectomy due to the spleen being unsalvageable. Post-operatively, the patient was admitted to the high-dependency unit (HDU) for close monitoring. Histological examination of the splenic tissue revealed B-cell lymphoid hyperplasia and negative PCR for clonality. The patient was found to be IgG-positive for mumps and was not vaccinated for MMR. Surgeons believe it is the main cause of ASR, given that little literature available establishes the same. The case highlights the importance of consideration of ASR in patients presenting with unexplained abdominal pain and hemodynamic instability, even without evidence of trauma. Early imaging and operative intervention are lifesaving. The histologic findings indicate that there may be an associated hemopoietic disorder, and this case highlights the need for clinicians to consider splenic involvement in patients with mumps who present with abdominal pain or signs of hemodynamic instability.</p>","PeriodicalId":93960,"journal":{"name":"Cureus","volume":"16 10","pages":"e72671"},"PeriodicalIF":1.3000,"publicationDate":"2024-10-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11523189/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cureus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7759/cureus.72671","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
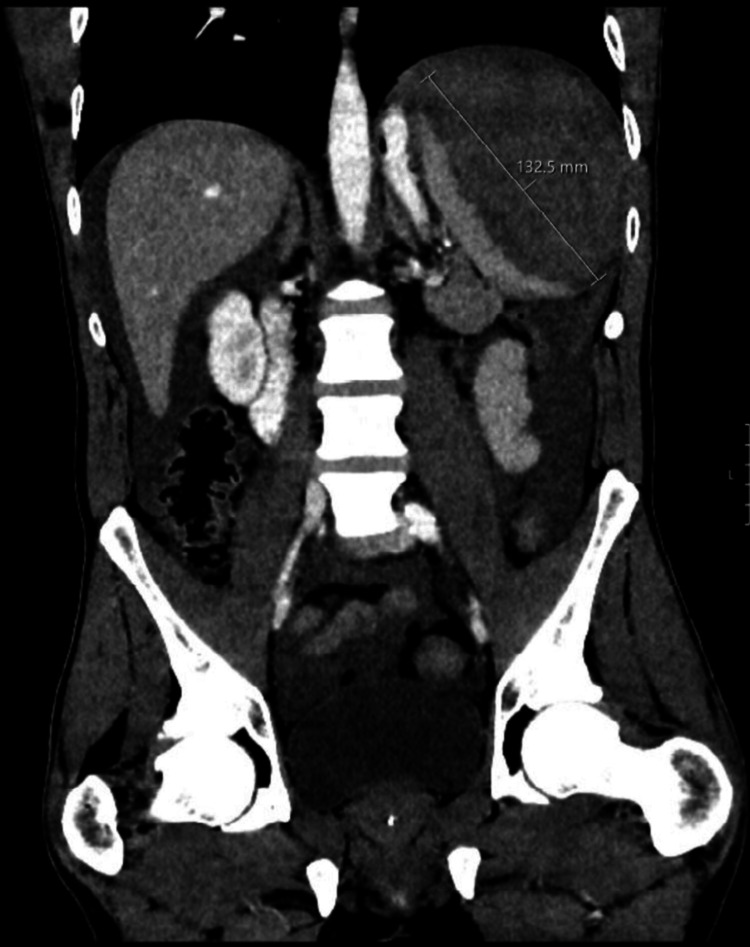
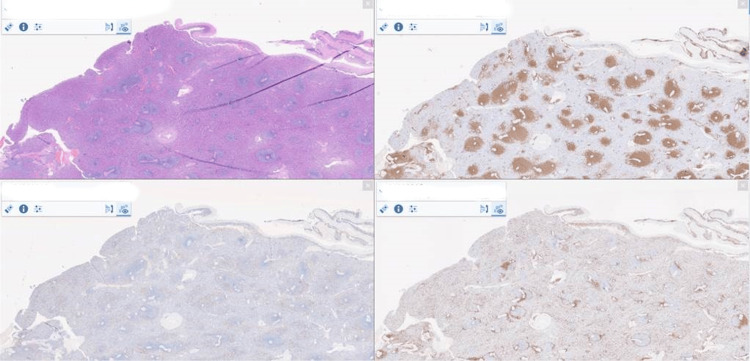
Atraumatic splenic rupture (ASR) is an unfamiliar entity that is potentially life-threatening if there is a delay in the diagnosis. Due to its rarity and its non-specific presentation, it can be a challenge to diagnose early. In this report, we present a case of a 42-year-old male patient who presented to the emergency department with nonspecific abdominal pain and had no past medical history. The patient presented abdominal pain associated with nausea, vomiting, and sweating. On examination, the patient was found to be tachycardic and mildly hypotensive, with mild left upper quadrant tenderness, and a lactate of 4 mmol/L on venous blood gas analysis. He was urgently transferred to the resuscitation area, where resuscitation commenced. Further investigations revealed significant anemia. The contrast-enhanced CT of the abdomen performed revealed a 13-cm splenic hemostasis suggestive of non-traumatic splenic rupture. The patient lacked any history of blunt trauma or family history that could account for the splenic rupture. The patient was taken to the theatre by the surgical team as he remained unstable. He received four units of blood in the theatre and underwent splenectomy due to the spleen being unsalvageable. Post-operatively, the patient was admitted to the high-dependency unit (HDU) for close monitoring. Histological examination of the splenic tissue revealed B-cell lymphoid hyperplasia and negative PCR for clonality. The patient was found to be IgG-positive for mumps and was not vaccinated for MMR. Surgeons believe it is the main cause of ASR, given that little literature available establishes the same. The case highlights the importance of consideration of ASR in patients presenting with unexplained abdominal pain and hemodynamic instability, even without evidence of trauma. Early imaging and operative intervention are lifesaving. The histologic findings indicate that there may be an associated hemopoietic disorder, and this case highlights the need for clinicians to consider splenic involvement in patients with mumps who present with abdominal pain or signs of hemodynamic instability.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
