Mohsin Fayaz, Sarabjit Singh Chibber, Kaushal Deep Singh, Lamkordor Tyngkam, Amir Hela, Bipin Chaurasia
{"title":"Unprecedented journey to 650 transpedicular screws using freehand technique and intraoperative C-arm imaging with technical nuances.","authors":"Mohsin Fayaz, Sarabjit Singh Chibber, Kaushal Deep Singh, Lamkordor Tyngkam, Amir Hela, Bipin Chaurasia","doi":"10.4103/jcvjs.jcvjs_56_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Pedicle screw placement plays a crucial role in treating various cases such as fractures, scoliosis, degenerative spine issues, and kyphosis, reinforcing all three spinal columns simultaneously. While three-dimensional navigation-assisted pedicle screw placement is considered superior, the freehand technique relies on anatomical landmarks and tactile feedback, with observed low complication rates.</p><p><strong>Materials and methods: </strong>This was a prospective single-center study conducted over a period of 3 years. It included all patients of dorsal, lumbar, and sacral spinal instability of myriad etiology. Previously operated patients and sick obtunded patients were excluded from the study.</p><p><strong>Results: </strong>In our study, we included 102 patients including 62 (60.7%) males and 40 (39.2%) females. More than half of patients were young in the age group of 20-50 years. Our study population had a varied etiology with 43.1% of patients having vertebral column instability due to trauma. The other etiologies were spondylolisthesis and lumbar canal stenosis (39.2%), Pott's spine (11.7%), tumors (2.9%), and osteoporotic fractures (2.9%). Majority of patients (44.1%) presented with lower backache with radiculopathy. All the transpedicular screws inserted were evaluated by C-arm to assess for screw fixation. In the first year of our study, an average of 4 anteroposterior (AP) and 4 lateral C-arm X-ray shots were taken per screw placement. In the next year, an average of 3 AP and 3 lateral shots and finally in the last year of our study only 2 AP and 2 lateral C-arm X-ray shots were taken per screw placement. Out of 650 screws placed, 4 screws were identified to cause breach with maximum breaches in the lumbar spine fixation. In dorsal spine fixation, there was 1 lateral breach at D10. In lumbar spine fixation, there were 3 breaches: two medial one each at L4 and L5 and one anterior at L2 level. The various complications include wound infection, temporary and permanent neurological deficit, screw breakage, screw misplacement, cerebrospinal fluid leaks, nonunion, and spinal epidural hematoma.</p><p><strong>Conclusions: </strong>Our study has provided strong encouragement to persist with the freehand technique in transpedicular fixation surgeries after a certain number of cases given the minimal breaches and complications observed. There are subtle technical nuances as we increase the number of cases with less exposure of anatomical landmarks and X-rays. Success hinges on experience, adherence to technique, and thorough preoperative planning. Further research and extended follow-up periods are necessary to firmly establish this technique as the gold standard.</p>","PeriodicalId":51721,"journal":{"name":"Journal of Craniovertebral Junction and Spine","volume":"15 3","pages":"326-330"},"PeriodicalIF":1.3000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11524549/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Craniovertebral Junction and Spine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jcvjs.jcvjs_56_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/12 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Pedicle screw placement plays a crucial role in treating various cases such as fractures, scoliosis, degenerative spine issues, and kyphosis, reinforcing all three spinal columns simultaneously. While three-dimensional navigation-assisted pedicle screw placement is considered superior, the freehand technique relies on anatomical landmarks and tactile feedback, with observed low complication rates.
Materials and methods: This was a prospective single-center study conducted over a period of 3 years. It included all patients of dorsal, lumbar, and sacral spinal instability of myriad etiology. Previously operated patients and sick obtunded patients were excluded from the study.
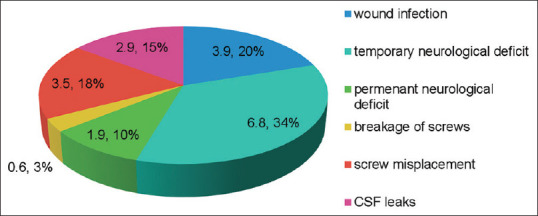
Results: In our study, we included 102 patients including 62 (60.7%) males and 40 (39.2%) females. More than half of patients were young in the age group of 20-50 years. Our study population had a varied etiology with 43.1% of patients having vertebral column instability due to trauma. The other etiologies were spondylolisthesis and lumbar canal stenosis (39.2%), Pott's spine (11.7%), tumors (2.9%), and osteoporotic fractures (2.9%). Majority of patients (44.1%) presented with lower backache with radiculopathy. All the transpedicular screws inserted were evaluated by C-arm to assess for screw fixation. In the first year of our study, an average of 4 anteroposterior (AP) and 4 lateral C-arm X-ray shots were taken per screw placement. In the next year, an average of 3 AP and 3 lateral shots and finally in the last year of our study only 2 AP and 2 lateral C-arm X-ray shots were taken per screw placement. Out of 650 screws placed, 4 screws were identified to cause breach with maximum breaches in the lumbar spine fixation. In dorsal spine fixation, there was 1 lateral breach at D10. In lumbar spine fixation, there were 3 breaches: two medial one each at L4 and L5 and one anterior at L2 level. The various complications include wound infection, temporary and permanent neurological deficit, screw breakage, screw misplacement, cerebrospinal fluid leaks, nonunion, and spinal epidural hematoma.
Conclusions: Our study has provided strong encouragement to persist with the freehand technique in transpedicular fixation surgeries after a certain number of cases given the minimal breaches and complications observed. There are subtle technical nuances as we increase the number of cases with less exposure of anatomical landmarks and X-rays. Success hinges on experience, adherence to technique, and thorough preoperative planning. Further research and extended follow-up periods are necessary to firmly establish this technique as the gold standard.






 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
