Allogeneic Hematopoietic Stem Cell Transplantation After Solid Organ Transplantation in Patients With Hematologic Malignancies Managed With Post-Transplant Cyclophosphamide-Based Graft-Versus-Host Disease Prophylaxis.
{"title":"Allogeneic Hematopoietic Stem Cell Transplantation After Solid Organ Transplantation in Patients With Hematologic Malignancies Managed With Post-Transplant Cyclophosphamide-Based Graft-Versus-Host Disease Prophylaxis.","authors":"Charley Jang, Jingmei Hsu","doi":"10.14740/jh1327","DOIUrl":null,"url":null,"abstract":"<p><p>Patients who receive solid organ transplants often require lifelong immunosuppression, which increases their risk for hematologic disorders. Allogeneic hematopoietic stem cell transplantation (HSCT) offers a potential curative treatment option for these patients. However, there is still a lack of understanding and guidance on graft-vs-host disease (GVHD) immunosuppression regimens, potential complications, and outcomes in patients with solid organ transplants who undergo HSCT. The rate of solid organ transplantation continues to increase annually, making this a common clinical scenario that hematologists encounter. In this case series, we present three patients who underwent liver, kidney and cardiac transplants and each developed hematological malignancies requiring allogeneic stem cell transplant. This is the first case report of two patients who received post-transplant cyclophosphamide with mycophenolate mofetil and tacrolimus GVHD prophylaxis. We also review recent advances in GVHD prophylaxis in allogeneic HSCT and solid organ transplantation including immune tolerance and immunosuppression-free protocols. Our case series support the use of post-transplant cyclophosphamide with mycophenolate mofetil and tacrolimus as post-transplant GVHD prophylaxis, which does not appear to compromise solid organ graft function. Our case series also provides evidence that allogeneic HSCT is a feasible and potentially life-saving treatment option in patients who develop hematologic malignancies after solid organ transplantation.</p>","PeriodicalId":15964,"journal":{"name":"Journal of hematology","volume":"13 5","pages":"250-258"},"PeriodicalIF":1.3000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11526586/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jh1327","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/21 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
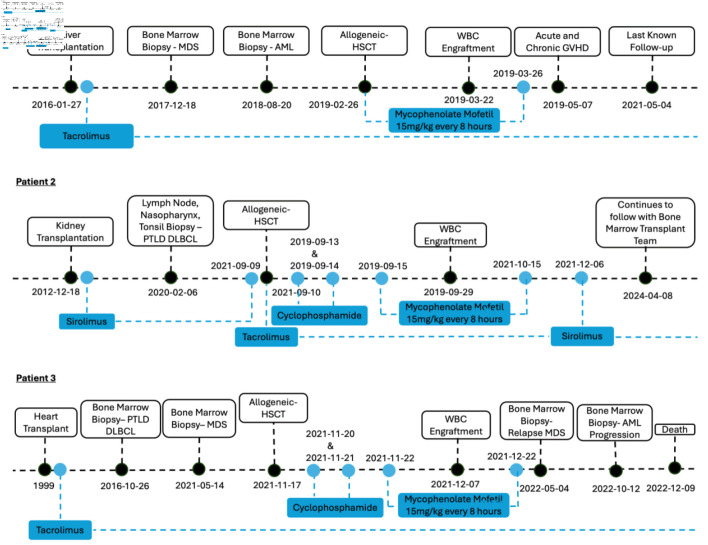
Patients who receive solid organ transplants often require lifelong immunosuppression, which increases their risk for hematologic disorders. Allogeneic hematopoietic stem cell transplantation (HSCT) offers a potential curative treatment option for these patients. However, there is still a lack of understanding and guidance on graft-vs-host disease (GVHD) immunosuppression regimens, potential complications, and outcomes in patients with solid organ transplants who undergo HSCT. The rate of solid organ transplantation continues to increase annually, making this a common clinical scenario that hematologists encounter. In this case series, we present three patients who underwent liver, kidney and cardiac transplants and each developed hematological malignancies requiring allogeneic stem cell transplant. This is the first case report of two patients who received post-transplant cyclophosphamide with mycophenolate mofetil and tacrolimus GVHD prophylaxis. We also review recent advances in GVHD prophylaxis in allogeneic HSCT and solid organ transplantation including immune tolerance and immunosuppression-free protocols. Our case series support the use of post-transplant cyclophosphamide with mycophenolate mofetil and tacrolimus as post-transplant GVHD prophylaxis, which does not appear to compromise solid organ graft function. Our case series also provides evidence that allogeneic HSCT is a feasible and potentially life-saving treatment option in patients who develop hematologic malignancies after solid organ transplantation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
