Invasive Versus Conservative Strategy in Older Adults ≥75 Years of Age With Non-ST-segment-Elevation Acute Coronary Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.
Amit Rout, Mohamad B Moumneh, Kriti Kalra, Sahib Singh, Aakash Garg, Vijay Kunadian, Simone Biscaglia, Mohamad A Alkhouli, Jennifer A Rymer, Wayne B Batchelor, Michael G Nanna, Abdulla A Damluji
{"title":"Invasive Versus Conservative Strategy in Older Adults ≥75 Years of Age With Non-ST-segment-Elevation Acute Coronary Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.","authors":"Amit Rout, Mohamad B Moumneh, Kriti Kalra, Sahib Singh, Aakash Garg, Vijay Kunadian, Simone Biscaglia, Mohamad A Alkhouli, Jennifer A Rymer, Wayne B Batchelor, Michael G Nanna, Abdulla A Damluji","doi":"10.1161/JAHA.124.036151","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Older adults with non-ST-segment-elevation acute coronary syndrome are less likely to undergo an invasive strategy compared with younger patients. Randomized controlled trials traditionally exclude older adults because of their high burden of geriatric conditions.</p><p><strong>Methods and results: </strong>We searched for randomized controlled trials comparing invasive versus medical management or a selective invasive (conservative) strategy for older patients (age≥75 years) with non-ST-segment-elevation acute coronary syndrome. Fixed effects meta-analysis was conducted to estimate the odds ratio (OR) with 95% CI for the composite of death or myocardial infarction (MI) and individual secondary end points of all-cause death, cardiovascular death, MI, revascularization, stroke, and major bleeding. Nine studies with 2429 patients (invasive: 1228 versus control: 1201) with a mean follow-up of 21 months were included. An invasive strategy was associated with a significantly decreased risk of a composite of death and MI (OR, 0.67 [95% CI, 0.54-0.83], <i>P</i><0.001), MI (OR, 0.56 [95% CI, 0.45-0.70], <i>P</i><0.001) and subsequent revascularization (OR, 0.27 [95% CI, 0.16-0.48], <i>P</i><0.001). There was no difference in all-cause death (OR, 0.84 [95% CI, 0.65-1.10], <i>P</i>=0.21), cardiovascular death (OR, 0.85 [95% CI, 0.63-1.15], <i>P</i>=0.30), stroke (OR, 0.74 [95% CI, 0.38-1.47], <i>P</i>=0.39), or major bleeding (OR, 1.24 [95% CI, 0.42-3.66], <i>P</i>=0.70).</p><p><strong>Conclusions: </strong>In older patients ≥75 years old with non-ST-segment-elevation acute coronary syndrome, an invasive strategy reduced the risk of a composite of death and MI, MI, and subsequent revascularization compared with a conservative strategy alone. Older adults with higher burden of geriatric conditions should be included in future trials to improve generalizability to this growing population.</p>","PeriodicalId":54370,"journal":{"name":"Journal of the American Heart Association","volume":" ","pages":"e036151"},"PeriodicalIF":5.3000,"publicationDate":"2024-11-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11935716/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Heart Association","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1161/JAHA.124.036151","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/4 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Older adults with non-ST-segment-elevation acute coronary syndrome are less likely to undergo an invasive strategy compared with younger patients. Randomized controlled trials traditionally exclude older adults because of their high burden of geriatric conditions.
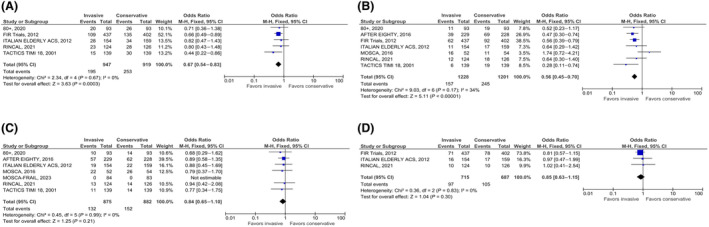
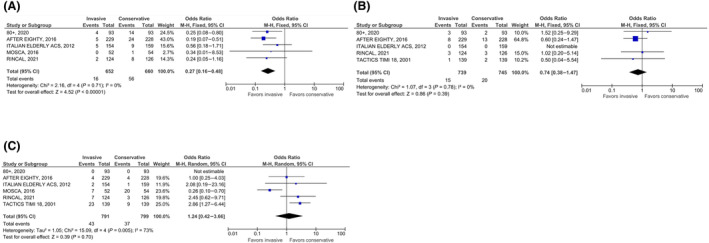
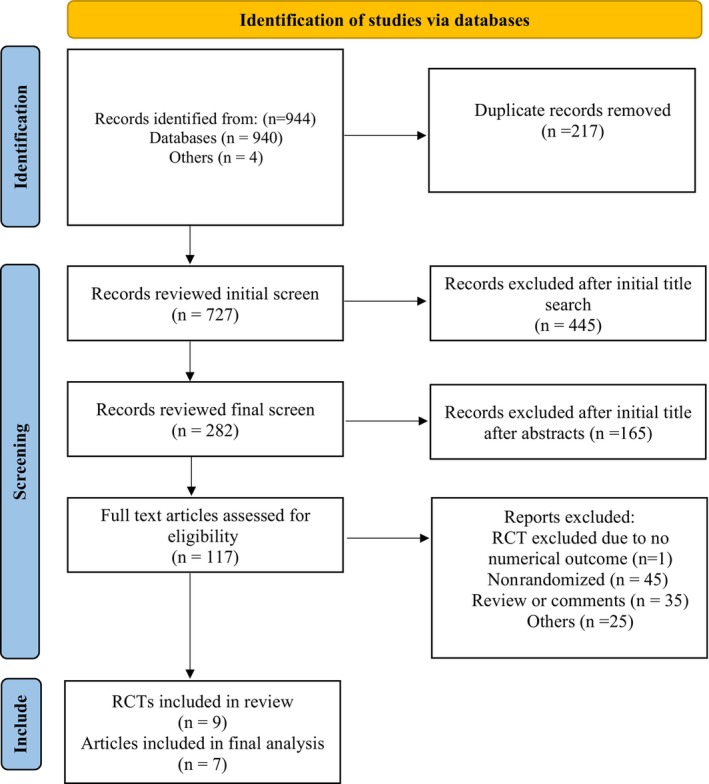
Methods and results: We searched for randomized controlled trials comparing invasive versus medical management or a selective invasive (conservative) strategy for older patients (age≥75 years) with non-ST-segment-elevation acute coronary syndrome. Fixed effects meta-analysis was conducted to estimate the odds ratio (OR) with 95% CI for the composite of death or myocardial infarction (MI) and individual secondary end points of all-cause death, cardiovascular death, MI, revascularization, stroke, and major bleeding. Nine studies with 2429 patients (invasive: 1228 versus control: 1201) with a mean follow-up of 21 months were included. An invasive strategy was associated with a significantly decreased risk of a composite of death and MI (OR, 0.67 [95% CI, 0.54-0.83], P<0.001), MI (OR, 0.56 [95% CI, 0.45-0.70], P<0.001) and subsequent revascularization (OR, 0.27 [95% CI, 0.16-0.48], P<0.001). There was no difference in all-cause death (OR, 0.84 [95% CI, 0.65-1.10], P=0.21), cardiovascular death (OR, 0.85 [95% CI, 0.63-1.15], P=0.30), stroke (OR, 0.74 [95% CI, 0.38-1.47], P=0.39), or major bleeding (OR, 1.24 [95% CI, 0.42-3.66], P=0.70).
Conclusions: In older patients ≥75 years old with non-ST-segment-elevation acute coronary syndrome, an invasive strategy reduced the risk of a composite of death and MI, MI, and subsequent revascularization compared with a conservative strategy alone. Older adults with higher burden of geriatric conditions should be included in future trials to improve generalizability to this growing population.
期刊介绍:
As an Open Access journal, JAHA - Journal of the American Heart Association is rapidly and freely available, accelerating the translation of strong science into effective practice.
JAHA is an authoritative, peer-reviewed Open Access journal focusing on cardiovascular and cerebrovascular disease. JAHA provides a global forum for basic and clinical research and timely reviews on cardiovascular disease and stroke. As an Open Access journal, its content is free on publication to read, download, and share, accelerating the translation of strong science into effective practice.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
