Syed Hasham Ali, Zoaib Habib Tharwani, Asad Ali Siddiqui, Fizza Iqbal, Mahnoor Sadiq, Ali Abdullah, Abdullah Khalid, Huzaifa Ul Haq Ansari, Muhammad Usman, Shurjeel Uddin Qazi, Uzair Munaf, Ibtehaj Ul Haque, Shayan Marsia
{"title":"Decompressive craniectomy versus craniotomy for acute subdural hematoma: A systematic review and meta-analysis with an adjusted subgroup analysis.","authors":"Syed Hasham Ali, Zoaib Habib Tharwani, Asad Ali Siddiqui, Fizza Iqbal, Mahnoor Sadiq, Ali Abdullah, Abdullah Khalid, Huzaifa Ul Haq Ansari, Muhammad Usman, Shurjeel Uddin Qazi, Uzair Munaf, Ibtehaj Ul Haque, Shayan Marsia","doi":"10.1177/11795735241297250","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Acute subdural hematomas are major causes of morbidity which warrant immediate treatment. If surgical intervention is warranted, craniotomy (CO) and decompressive craniectomy (DC) are employed, largely based on a loosely defined criteria and the neurosurgeon's best judgment. The primacy of one approach over another is a matter of dispute.</p><p><strong>Objective: </strong>We attempt to further clarify any advantages in the two techniques, and include a propensity score matched (PSM) subgroup analysis to eliminate bias.</p><p><strong>Design: </strong>This meta-analysis was conducted following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines.</p><p><strong>Data sources and methods: </strong>A literature review was conducted on PubMed/Medline, Cochrane Central, and Google Scholar from inception to September 2023. 15 studies were extracted, and three outcomes were meta-analyzed: Mortality, Glasgow Outcome Scale (GOS) scores and patients undergoing re-operations/revisions. Odds Ratios (OR) and Mean Difference (MD) were used in dichotomous and continuous variables respectively. PSM data was used wherever possible. A subgroup analysis was conducted with 5 PSM studies and a trial. Heterogeneity was addressed if above 40% and the <i>P</i>-value is significant (≤ .05).</p><p><strong>Results: </strong>A total of 15 studies were meta-analyzed with a total of 2327 and 2171 patients undergoing CO and DC respectively. Patients undergoing DC had a significantly worse GOS 5 outcome (OR: .63 [95% CI: .45-.87]; <i>P</i> = .005; I2 = 0%) and higher mortality (OR: 1.58 [95% CI: 1.20-2.08]; <i>P</i> = .001; I2 = 67%). In subgroup analysis of adjusted studies, DC still had significantly higher mortality. (OR: 1.50 [95% CI: 1.03-2.18]; <i>P</i> = .001; I2 = 83%).</p><p><strong>Conclusions: </strong>This meta-analysis determines that CO is more viable than DC as a surgical option due to its less invasive nature. DC can be employed, albeit under strict preprocedural patient selection and for highly specific indications.</p>","PeriodicalId":15218,"journal":{"name":"Journal of Central Nervous System Disease","volume":"16 ","pages":"11795735241297250"},"PeriodicalIF":2.8000,"publicationDate":"2024-11-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11533180/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Central Nervous System Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795735241297250","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
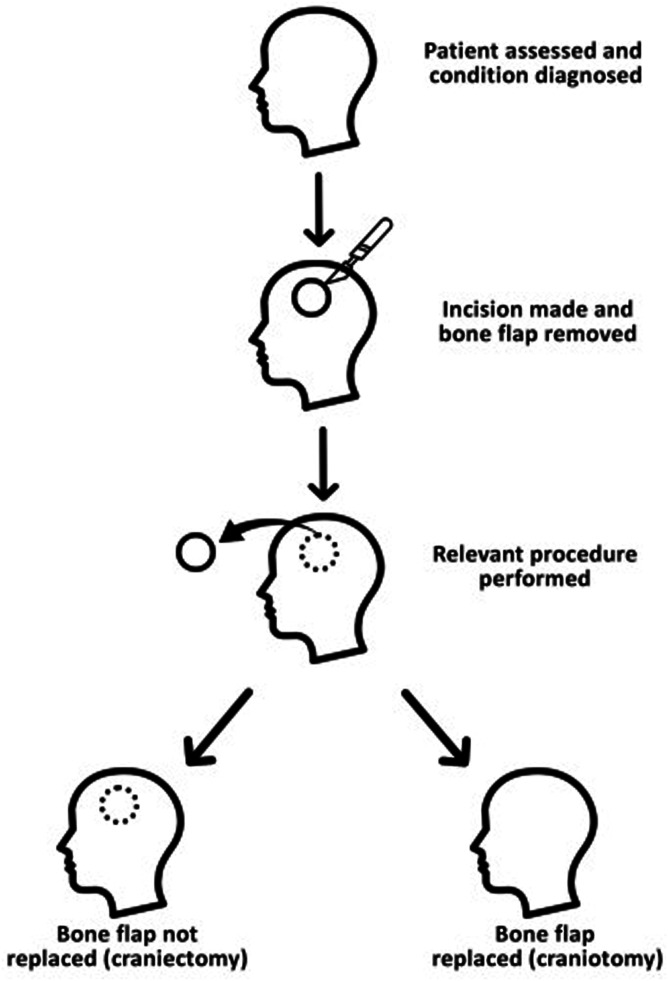
Introduction: Acute subdural hematomas are major causes of morbidity which warrant immediate treatment. If surgical intervention is warranted, craniotomy (CO) and decompressive craniectomy (DC) are employed, largely based on a loosely defined criteria and the neurosurgeon's best judgment. The primacy of one approach over another is a matter of dispute.
Objective: We attempt to further clarify any advantages in the two techniques, and include a propensity score matched (PSM) subgroup analysis to eliminate bias.
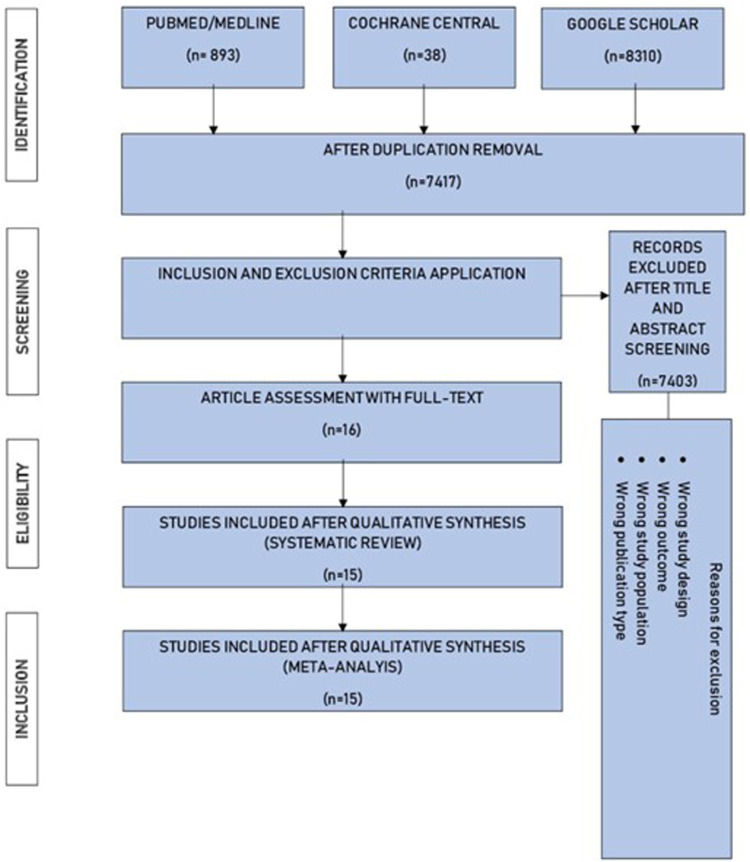
Design: This meta-analysis was conducted following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines.
Data sources and methods: A literature review was conducted on PubMed/Medline, Cochrane Central, and Google Scholar from inception to September 2023. 15 studies were extracted, and three outcomes were meta-analyzed: Mortality, Glasgow Outcome Scale (GOS) scores and patients undergoing re-operations/revisions. Odds Ratios (OR) and Mean Difference (MD) were used in dichotomous and continuous variables respectively. PSM data was used wherever possible. A subgroup analysis was conducted with 5 PSM studies and a trial. Heterogeneity was addressed if above 40% and the P-value is significant (≤ .05).
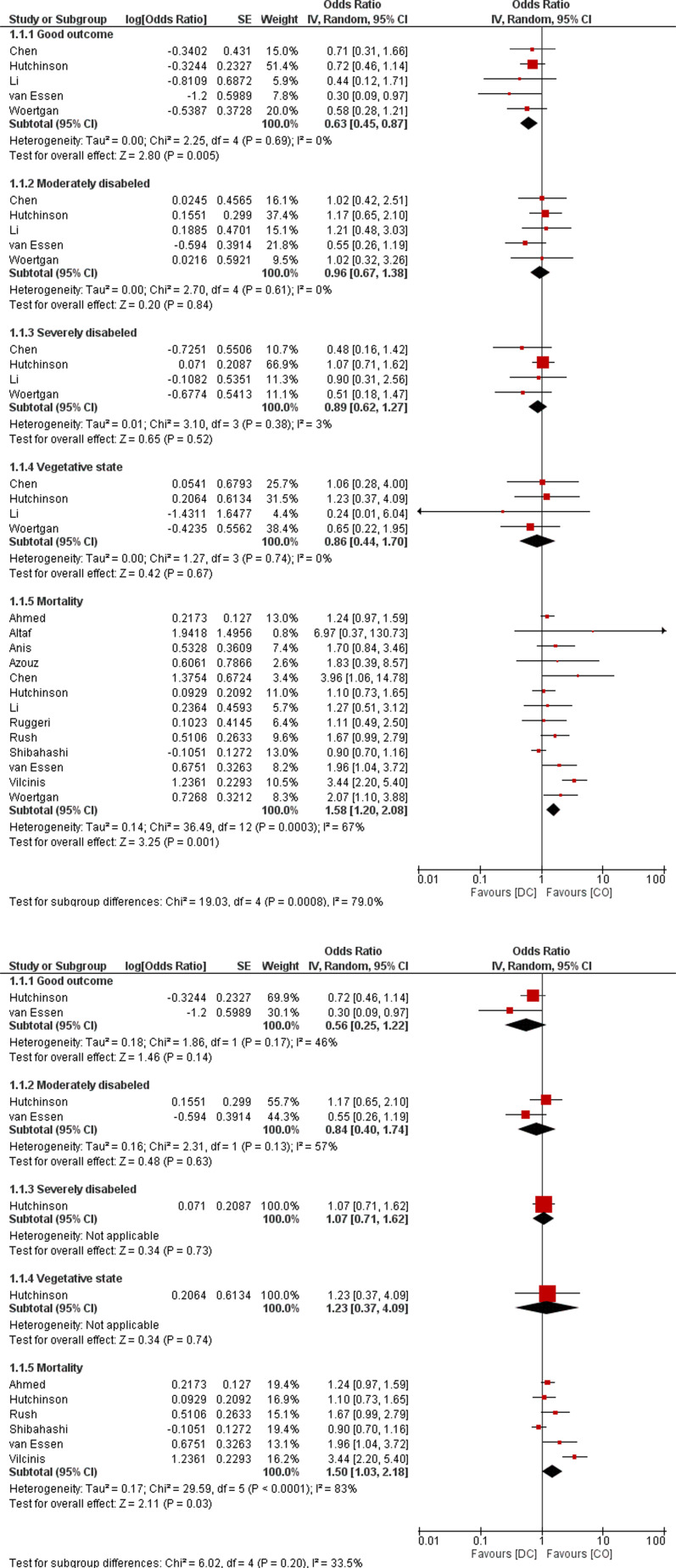
Results: A total of 15 studies were meta-analyzed with a total of 2327 and 2171 patients undergoing CO and DC respectively. Patients undergoing DC had a significantly worse GOS 5 outcome (OR: .63 [95% CI: .45-.87]; P = .005; I2 = 0%) and higher mortality (OR: 1.58 [95% CI: 1.20-2.08]; P = .001; I2 = 67%). In subgroup analysis of adjusted studies, DC still had significantly higher mortality. (OR: 1.50 [95% CI: 1.03-2.18]; P = .001; I2 = 83%).
Conclusions: This meta-analysis determines that CO is more viable than DC as a surgical option due to its less invasive nature. DC can be employed, albeit under strict preprocedural patient selection and for highly specific indications.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
