Sairi Zhang, J Anthony Chacko, Riley N Sanders, Eric R Rosenbaum, Philip W Dockery, Ahmed B Sallam
{"title":"Progression of Sclerouveitis to Endogenous <i>Fusarium</i> Endophthalmitis.","authors":"Sairi Zhang, J Anthony Chacko, Riley N Sanders, Eric R Rosenbaum, Philip W Dockery, Ahmed B Sallam","doi":"10.1155/2024/5549818","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction:</b> We describe a unique case of sclerouveitis that progressed to endogenous <i>Fusarium</i> endophthalmitis in a 69-year-old male with chronic lymphocytic leukemia (CLL). We highlight the risk of treating sclerouveitis with oral corticosteroids, which can exacerbate an infection and contribute to disease progression. <b>Case Presentation:</b> A 69-year-old male with CLL on zanubrutinib, a second-generation Bruton's tyrosine kinase inhibitor, was admitted to the hospital for osteomyelitis of the left foot. At presentation, the patient also reported right eye pain for 1 week and vision loss over the course of 1 month. Vision in the right eye was hand motion. Slit lamp examination revealed scleral inflammation in the right eye with violaceous injection, chemosis, inflammation in the anterior chamber, and diffuse subconjunctival hemorrhage. There was significant corneal edema preventing fundus examination. B-scan ultrasonography demonstrated a flat retina with no vitritis or scleral thickening. Forty-eight hours after treatment with oral and topical corticosteroids, the patient's eye pain improved but his vision worsened. Repeat B-scan showed new-onset vitritis. Fungal culture obtained by diagnostic pars plana vitrectomy (PPV) revealed growth of <i>Fusarium</i>. The patient was treated with oral and intravitreal voriconazole in addition to intravenous voriconazole and amphotericin B for systemic therapy. Corticosteroids were discontinued. Despite aggressive therapy, the patient's disposition declined to the point of transitioning to comfort-focused care, and he passed away. <b>Conclusion:</b> Endogenous fungal endophthalmitis is most commonly seen in immunocompromised patients, and oral corticosteroid therapy for such patients should be used with caution as it can worsen an infection. In cases of fusarial endophthalmitis, visual prognosis is poor.</p>","PeriodicalId":9603,"journal":{"name":"Case Reports in Ophthalmological Medicine","volume":"2024 ","pages":"5549818"},"PeriodicalIF":0.4000,"publicationDate":"2024-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11535266/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Ophthalmological Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/5549818","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
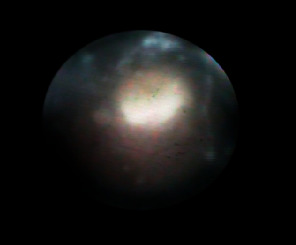
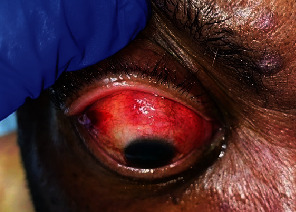
Introduction: We describe a unique case of sclerouveitis that progressed to endogenous Fusarium endophthalmitis in a 69-year-old male with chronic lymphocytic leukemia (CLL). We highlight the risk of treating sclerouveitis with oral corticosteroids, which can exacerbate an infection and contribute to disease progression. Case Presentation: A 69-year-old male with CLL on zanubrutinib, a second-generation Bruton's tyrosine kinase inhibitor, was admitted to the hospital for osteomyelitis of the left foot. At presentation, the patient also reported right eye pain for 1 week and vision loss over the course of 1 month. Vision in the right eye was hand motion. Slit lamp examination revealed scleral inflammation in the right eye with violaceous injection, chemosis, inflammation in the anterior chamber, and diffuse subconjunctival hemorrhage. There was significant corneal edema preventing fundus examination. B-scan ultrasonography demonstrated a flat retina with no vitritis or scleral thickening. Forty-eight hours after treatment with oral and topical corticosteroids, the patient's eye pain improved but his vision worsened. Repeat B-scan showed new-onset vitritis. Fungal culture obtained by diagnostic pars plana vitrectomy (PPV) revealed growth of Fusarium. The patient was treated with oral and intravitreal voriconazole in addition to intravenous voriconazole and amphotericin B for systemic therapy. Corticosteroids were discontinued. Despite aggressive therapy, the patient's disposition declined to the point of transitioning to comfort-focused care, and he passed away. Conclusion: Endogenous fungal endophthalmitis is most commonly seen in immunocompromised patients, and oral corticosteroid therapy for such patients should be used with caution as it can worsen an infection. In cases of fusarial endophthalmitis, visual prognosis is poor.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
