Noa Krugliak Cleveland, Ninfa Candela, John A Carter, Maja Kuharic, Joyce Qian, Zhaoli Tang, Robin Turpin, David T Rubin
{"title":"Real-World Treatment Outcomes Associated With Early Versus Delayed Vedolizumab Initiation in Patients With Ulcerative Colitis.","authors":"Noa Krugliak Cleveland, Ninfa Candela, John A Carter, Maja Kuharic, Joyce Qian, Zhaoli Tang, Robin Turpin, David T Rubin","doi":"10.1093/crocol/otae061","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with ulcerative colitis (UC) typically receive a targeted inflammatory bowel disease therapy after treatment with conventional therapies and after the development of significant morbidity. Evidence suggests that early biologic treatment after diagnosis could improve treatment response and prevent disease complications compared with delayed biologic treatment after conventional therapy.</p><p><strong>Methods: </strong>RALEE was a retrospective study using claims data from IBM® MarketScan® Research Databases between January 1, 2016 and December 31, 2019. Adults with UC and at least one claim for vedolizumab were categorized into Early or Delayed Vedolizumab groups according to whether they had received vedolizumab within 30 days of diagnosis or after conventional therapy (5-aminosalicylates, corticosteroids, and immunomodulators), respectively. Treatment response was assessed at 2, 6, and 12 months after vedolizumab treatment initiation and was analyzed with logistic regression (bivariate).</p><p><strong>Results: </strong>At 2 months, Delayed Vedolizumab was associated with significantly higher odds of nonresponse than Early Vedolizumab (odds ratio [OR], 2.509; 95% confidence interval [CI], 1.28-4.90). Delayed Vedolizumab was not significantly associated with odds of nonresponse at 6 months (OR, 1.173; 95% CI, 0.72-1.90) or at 12 months (OR, 0.872; 95% CI, 0.55-1.37). Mean total healthcare costs were similar in the Early Vedolizumab ($6492) and Delayed Vedolizumab ($5897) groups, although there were small differences in costs from different types of claims.</p><p><strong>Conclusions: </strong>Patients who received vedolizumab early after UC diagnosis were less likely to experience nonresponse at 2 months and incurred similar healthcare costs at 12 months compared with patients who received delayed vedolizumab.</p>","PeriodicalId":10847,"journal":{"name":"Crohn's & Colitis 360","volume":"6 4","pages":"otae061"},"PeriodicalIF":1.8000,"publicationDate":"2024-10-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11535256/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Crohn's & Colitis 360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/crocol/otae061","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patients with ulcerative colitis (UC) typically receive a targeted inflammatory bowel disease therapy after treatment with conventional therapies and after the development of significant morbidity. Evidence suggests that early biologic treatment after diagnosis could improve treatment response and prevent disease complications compared with delayed biologic treatment after conventional therapy.
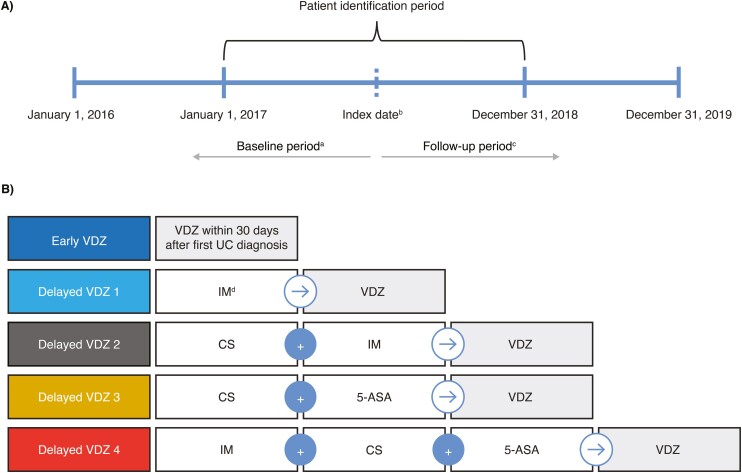
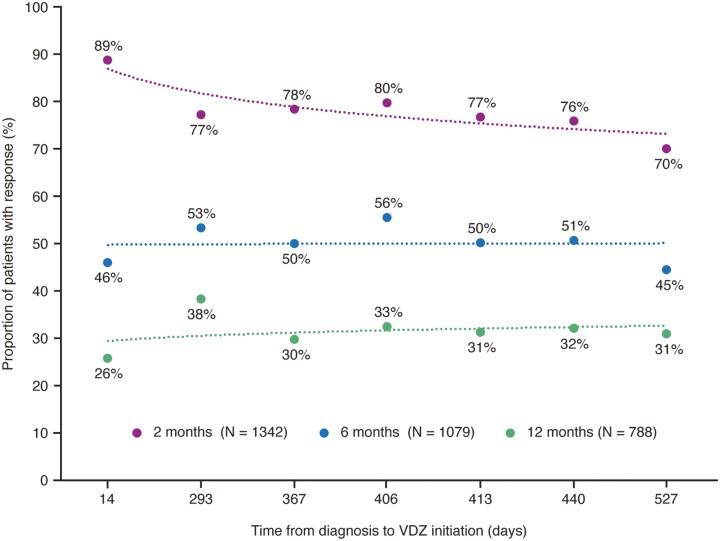
Methods: RALEE was a retrospective study using claims data from IBM® MarketScan® Research Databases between January 1, 2016 and December 31, 2019. Adults with UC and at least one claim for vedolizumab were categorized into Early or Delayed Vedolizumab groups according to whether they had received vedolizumab within 30 days of diagnosis or after conventional therapy (5-aminosalicylates, corticosteroids, and immunomodulators), respectively. Treatment response was assessed at 2, 6, and 12 months after vedolizumab treatment initiation and was analyzed with logistic regression (bivariate).
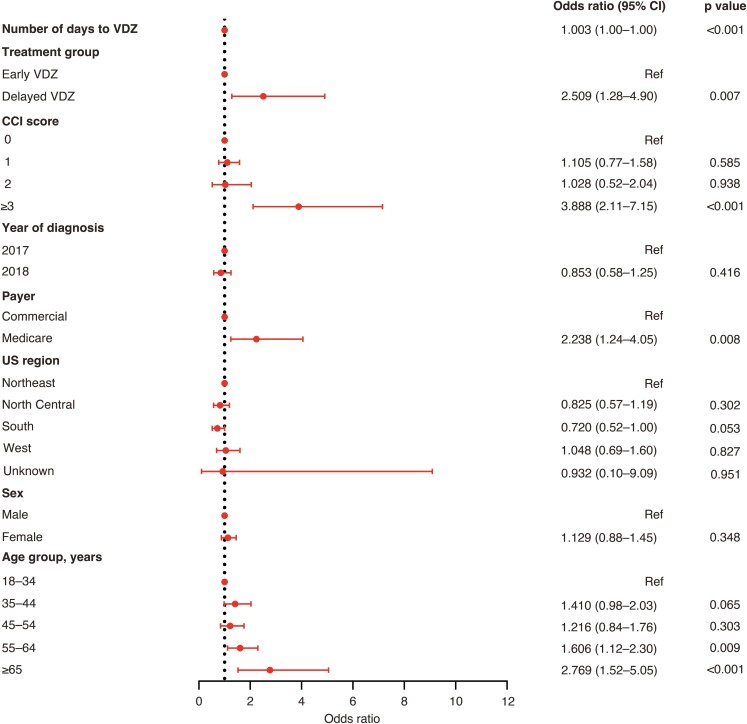
Results: At 2 months, Delayed Vedolizumab was associated with significantly higher odds of nonresponse than Early Vedolizumab (odds ratio [OR], 2.509; 95% confidence interval [CI], 1.28-4.90). Delayed Vedolizumab was not significantly associated with odds of nonresponse at 6 months (OR, 1.173; 95% CI, 0.72-1.90) or at 12 months (OR, 0.872; 95% CI, 0.55-1.37). Mean total healthcare costs were similar in the Early Vedolizumab ($6492) and Delayed Vedolizumab ($5897) groups, although there were small differences in costs from different types of claims.
Conclusions: Patients who received vedolizumab early after UC diagnosis were less likely to experience nonresponse at 2 months and incurred similar healthcare costs at 12 months compared with patients who received delayed vedolizumab.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
