{"title":"Risk Classification of Patients With Advanced Urothelial Carcinoma Treated With Enfortumab Vedotin.","authors":"Gaku Ishikawa, Yuto Matsushita, Yuichi Kitagawa, Asuka Uchiyama, Yuya Oishi, Hiroki Tanaka, Shinya Watanabe, Eito Suzuki, Shunsuke Watanabe, Kyohei Watanabe, Hiromitsu Watanabe, Keita Tamura, Daisuke Motoyama, Rikiya Matsumoto, Toshiki Ito, Masao Nagata, Toshiyuki Unno, Hiroshi Furuse, Takuji Mizuno, Atsushi Otsuka","doi":"10.21873/cdp.10396","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aim: </strong>Enfortumab Vedotin (EV) is a widely used antibody-drug conjugate for patients with advanced urothelial carcinoma (UC) who have previously been treated with platinum-based chemotherapy and immune checkpoint inhibitors. However, limited information is currently available on prognostic factors and risk classification. Therefore, the present study attempted to identify clinical factors that predict outcomes in patients with advanced UC treated with EV and to develop a novel risk classification model.</p><p><strong>Patients and methods: </strong>We conducted a multicenter retrospective study including patients with advanced UC treated with EV. Oncological outcomes were assessed using progression-free survival (PFS) and overall survival (OS), and prognostic factors for PFS and OS were investigated. We then examined the usefulness of risk classification based on the prognostic factors identified.</p><p><strong>Results: </strong>Median PFS and OS were 7.1 and 16.3 months, respectively. High C-reactive protein levels (CRP level ≥0.5 mg/dl) and hypercalcemia (corrected calcium level >10.2 mg/dl) were identified as prognostic factors for PFS (p=0.012 and p=0.003, respectively) and OS (p=0.035 and p<0.001, respectively). We then divided patients into three risk groups: no prognostic factors group, one prognostic factor group, and two prognostic factors group. Significant differences were observed in PFS and OS among the three groups (p<0.001 and p<0.001, respectively) and c-indices were 0.766 for PFS and 0.800 for OS.</p><p><strong>Conclusion: </strong>The risk classification using CRP and hypercalcemia is useful for predicting the outcomes of patients with advanced UC treated with EV.</p>","PeriodicalId":72510,"journal":{"name":"Cancer diagnosis & prognosis","volume":"4 6","pages":"783-788"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11534046/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer diagnosis & prognosis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21873/cdp.10396","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background/aim: Enfortumab Vedotin (EV) is a widely used antibody-drug conjugate for patients with advanced urothelial carcinoma (UC) who have previously been treated with platinum-based chemotherapy and immune checkpoint inhibitors. However, limited information is currently available on prognostic factors and risk classification. Therefore, the present study attempted to identify clinical factors that predict outcomes in patients with advanced UC treated with EV and to develop a novel risk classification model.
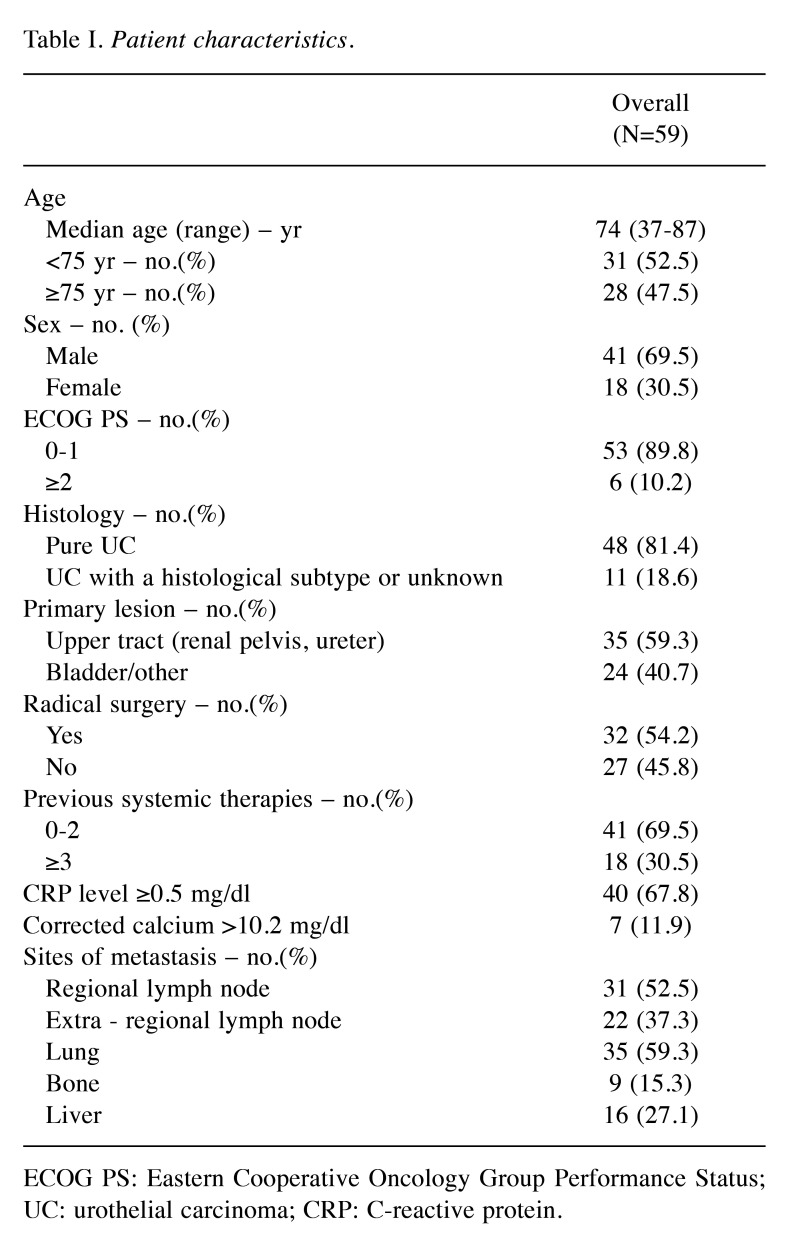
Patients and methods: We conducted a multicenter retrospective study including patients with advanced UC treated with EV. Oncological outcomes were assessed using progression-free survival (PFS) and overall survival (OS), and prognostic factors for PFS and OS were investigated. We then examined the usefulness of risk classification based on the prognostic factors identified.
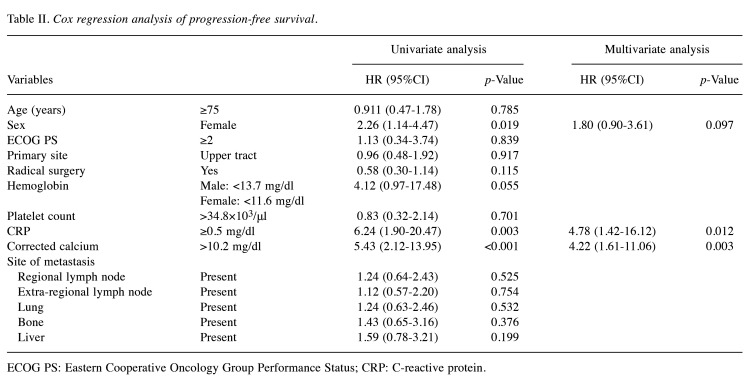
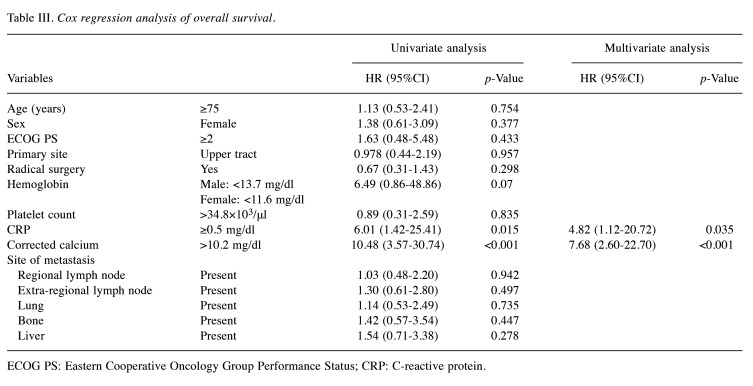
Results: Median PFS and OS were 7.1 and 16.3 months, respectively. High C-reactive protein levels (CRP level ≥0.5 mg/dl) and hypercalcemia (corrected calcium level >10.2 mg/dl) were identified as prognostic factors for PFS (p=0.012 and p=0.003, respectively) and OS (p=0.035 and p<0.001, respectively). We then divided patients into three risk groups: no prognostic factors group, one prognostic factor group, and two prognostic factors group. Significant differences were observed in PFS and OS among the three groups (p<0.001 and p<0.001, respectively) and c-indices were 0.766 for PFS and 0.800 for OS.
Conclusion: The risk classification using CRP and hypercalcemia is useful for predicting the outcomes of patients with advanced UC treated with EV.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
