Minna Järvensivu-Koivunen, Antti Kallonen, Mark van Gils, Leo-Pekka Lyytikäinen, Juho Tynkkynen, Jussi Hernesniemi
{"title":"Predicting long-term risk of sudden cardiac death with automatic computer-interpretations of electrocardiogram.","authors":"Minna Järvensivu-Koivunen, Antti Kallonen, Mark van Gils, Leo-Pekka Lyytikäinen, Juho Tynkkynen, Jussi Hernesniemi","doi":"10.3389/fcvm.2024.1439069","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Computer-interpreted electrocardiogram (CIE) data is provided by almost all commercial software used to capture and store digital electrocardiograms. CIE is widely available, inexpensive, and accurate. We tested the potential of CIE in long-term sudden cardiac death (SCD) risk prediction.</p><p><strong>Methods: </strong>This is a retrospective of 8,568 consecutive patients treated for acute coronary syndrome. The primary endpoint was five-year occurrence of SCDs or equivalent events (SCDs aborted by successful resuscitation or adequate ICD therapy). CIE statements were extracted from summary statements and measurements made by the GE Muse 12SL algorithm from ECGs taken during admission. Three supervised machine learning algorithms (logistic regression, extreme gradient boosting, and random forest) were then used for analysis to find risk features using a random 70/30% split for discovery and validation cohorts.</p><p><strong>Results: </strong>Five-year SCD occurrence rate was 3.3% (<i>n</i> = 287). Regardless of the used ML algorithm, the most significant risk ECG risk features detected by the CIE included known risk features such as QRS duration and factors associated with QRS duration, heart rate-corrected QT time (QTc), and the presence of premature ventricular contractions (PVCs). Risk score formed by using most significant CIE features associated with the risk of SCD despite adjusting for any clinical risk factor (including left ventricular ejection fraction). Sensitivity of CIE data to correctly identify patients with high risk of SCD (over 10% 5-year risk of SCD) was usually low, but specificity and negative prediction value reached up to 96.9% and 97.3% when selecting only the most significant features identified by logistic regression modeling (<i>p</i>-value threshold <0.01 for accepting features in the model). Overall, CIE data showed a modest overall performance for identifying high risk individuals with area under the receiver operating characteristic curve values ranging between 0.652 and 0.693 (highest for extreme gradient boosting and lowest for logistic regression).</p><p><strong>Conclusion: </strong>This proof-of-concept study shows that automatic interpretation of ECG identifies previously validated risk features for SCD.</p>","PeriodicalId":12414,"journal":{"name":"Frontiers in Cardiovascular Medicine","volume":"11 ","pages":"1439069"},"PeriodicalIF":2.8000,"publicationDate":"2024-10-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11537987/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Cardiovascular Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fcvm.2024.1439069","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
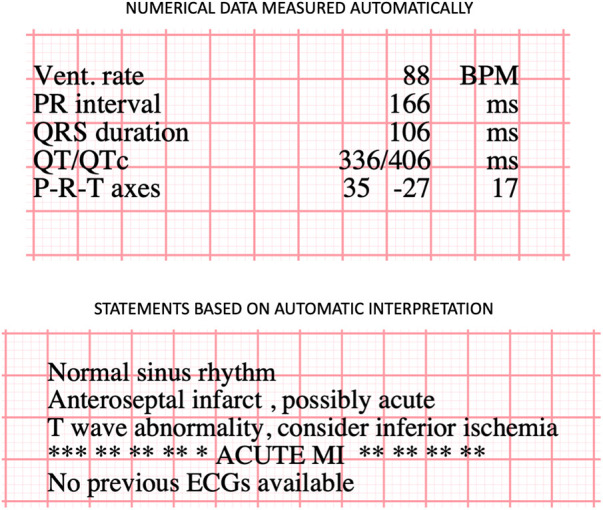
Background: Computer-interpreted electrocardiogram (CIE) data is provided by almost all commercial software used to capture and store digital electrocardiograms. CIE is widely available, inexpensive, and accurate. We tested the potential of CIE in long-term sudden cardiac death (SCD) risk prediction.
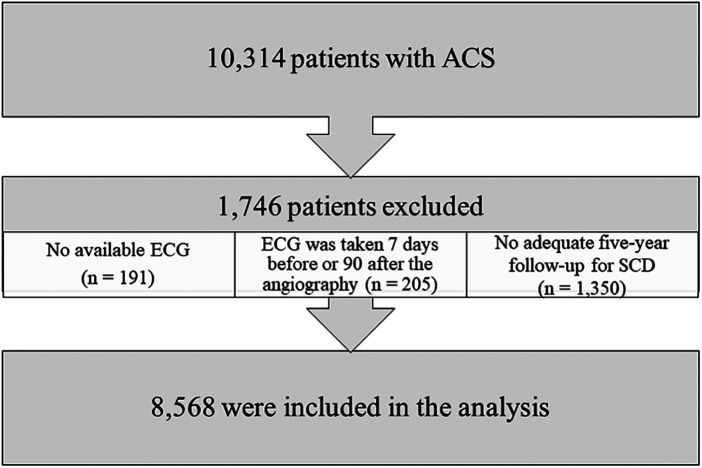
Methods: This is a retrospective of 8,568 consecutive patients treated for acute coronary syndrome. The primary endpoint was five-year occurrence of SCDs or equivalent events (SCDs aborted by successful resuscitation or adequate ICD therapy). CIE statements were extracted from summary statements and measurements made by the GE Muse 12SL algorithm from ECGs taken during admission. Three supervised machine learning algorithms (logistic regression, extreme gradient boosting, and random forest) were then used for analysis to find risk features using a random 70/30% split for discovery and validation cohorts.
Results: Five-year SCD occurrence rate was 3.3% (n = 287). Regardless of the used ML algorithm, the most significant risk ECG risk features detected by the CIE included known risk features such as QRS duration and factors associated with QRS duration, heart rate-corrected QT time (QTc), and the presence of premature ventricular contractions (PVCs). Risk score formed by using most significant CIE features associated with the risk of SCD despite adjusting for any clinical risk factor (including left ventricular ejection fraction). Sensitivity of CIE data to correctly identify patients with high risk of SCD (over 10% 5-year risk of SCD) was usually low, but specificity and negative prediction value reached up to 96.9% and 97.3% when selecting only the most significant features identified by logistic regression modeling (p-value threshold <0.01 for accepting features in the model). Overall, CIE data showed a modest overall performance for identifying high risk individuals with area under the receiver operating characteristic curve values ranging between 0.652 and 0.693 (highest for extreme gradient boosting and lowest for logistic regression).
Conclusion: This proof-of-concept study shows that automatic interpretation of ECG identifies previously validated risk features for SCD.
期刊介绍:
Frontiers? Which frontiers? Where exactly are the frontiers of cardiovascular medicine? And who should be defining these frontiers?
At Frontiers in Cardiovascular Medicine we believe it is worth being curious to foresee and explore beyond the current frontiers. In other words, we would like, through the articles published by our community journal Frontiers in Cardiovascular Medicine, to anticipate the future of cardiovascular medicine, and thus better prevent cardiovascular disorders and improve therapeutic options and outcomes of our patients.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
