Yan Chen, Ella X Du, Manasvi Sundar, Keith A Betts, Xin Yin, Samantha Eiffert, Karen Beauchamp, Andrew Delgado, Lisa Rosenblatt
{"title":"Costs of Adverse Events in Patients with Advanced or Metastatic Renal Cell Carcinoma with First-Line Treatment.","authors":"Yan Chen, Ella X Du, Manasvi Sundar, Keith A Betts, Xin Yin, Samantha Eiffert, Karen Beauchamp, Andrew Delgado, Lisa Rosenblatt","doi":"10.1007/s41669-024-00534-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>This study evaluated costs associated with adverse events (AEs) in previously untreated real-world patients with advanced renal cell carcinoma (aRCC) in the USA.</p><p><strong>Materials and methods: </strong>This retrospective longitudinal cohort study analyzed data from the Merative MarketScan Research Database (1 January 2014-30 September 2021). Adult patients with aRCC receiving first-line systemic treatments for aRCC (tyrosine kinase inhibitors [TKIs], or combination therapies of TKIs and immunotherapy) on or after the date of aRCC diagnosis were included. A total of 27 AEs of interest were included based on a review of product labels of the first-line treatments included in the study and identified using International Classification of Diseases, Ninth/Tenth Revision, Clinical Modification codes. Incremental costs associated with AEs between cases and controls (unadjusted and adjusted for relevant baseline characteristics) were estimated by two-part modeling. Analyses were performed over three AE cost assessment periods (7, 14, and 30 days).</p><p><strong>Results: </strong>The study included 1681 patients with aRCC (mean [standard deviation; SD] age, 60.8 [10.6] years; 73.1% male), of which 1542 (91.7%) had at least one AE. AEs were mostly diagnosed in the outpatient (OP) setting. For most AEs, cases had significantly higher unadjusted and adjusted costs than controls. Costs associated with AEs ranged from < 300 US dollars (USD) for proteinuria to nearly 60,000 USD for hypophosphatemia. Seventeen AEs had adjusted 30-day costs exceeding 10,000 USD; of these, nine (pancreatitis, acute kidney injury, dyspnea, hypotension, hyperkalemia, hypomagnesemia, hyponatremia, hypophosphatemia, and neutrophil decreased/neutropenia) had 30-day costs exceeding 20,000 USD.</p><p><strong>Limitations: </strong>The study was subject to limitations of all observational analyses of claims data (e.g., residual confounding). Observed cost differences may not have been solely attributable to an AE of interest. Study findings may not be generalizable to aRCC patient populations outside the USA.</p><p><strong>Conclusion: </strong>Most patients experienced at least one AE after initiation of first-line treatment with a TKI or combination therapies of TKIs and immunotherapy. There were substantial costs associated with AEs. Considering both safety and efficacy profiles when selecting optimal treatments can potentially mitigate healthcare costs for aRCC.</p>","PeriodicalId":19770,"journal":{"name":"PharmacoEconomics Open","volume":" ","pages":"125-136"},"PeriodicalIF":2.1000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11718028/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s41669-024-00534-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/6 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: This study evaluated costs associated with adverse events (AEs) in previously untreated real-world patients with advanced renal cell carcinoma (aRCC) in the USA.
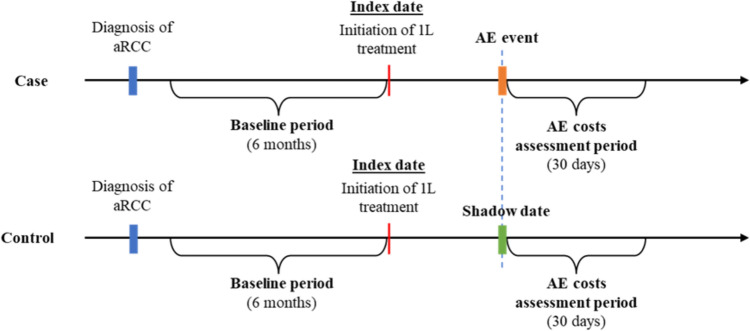
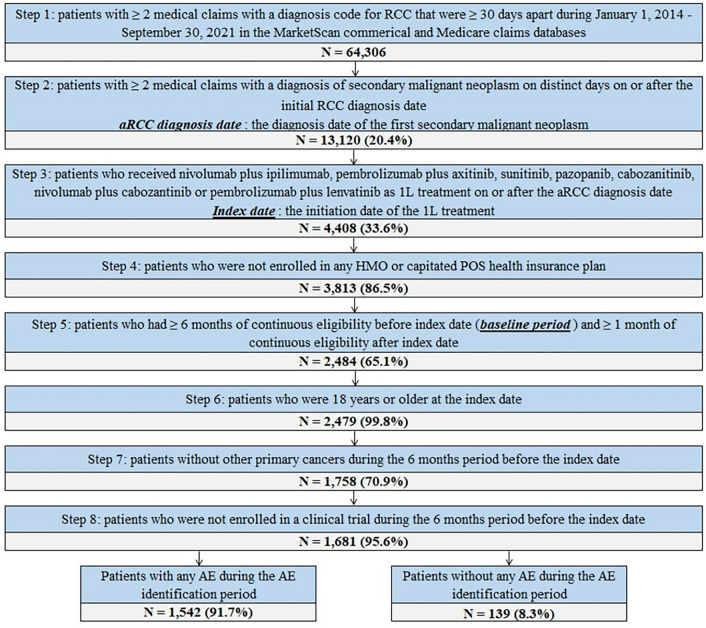
Materials and methods: This retrospective longitudinal cohort study analyzed data from the Merative MarketScan Research Database (1 January 2014-30 September 2021). Adult patients with aRCC receiving first-line systemic treatments for aRCC (tyrosine kinase inhibitors [TKIs], or combination therapies of TKIs and immunotherapy) on or after the date of aRCC diagnosis were included. A total of 27 AEs of interest were included based on a review of product labels of the first-line treatments included in the study and identified using International Classification of Diseases, Ninth/Tenth Revision, Clinical Modification codes. Incremental costs associated with AEs between cases and controls (unadjusted and adjusted for relevant baseline characteristics) were estimated by two-part modeling. Analyses were performed over three AE cost assessment periods (7, 14, and 30 days).
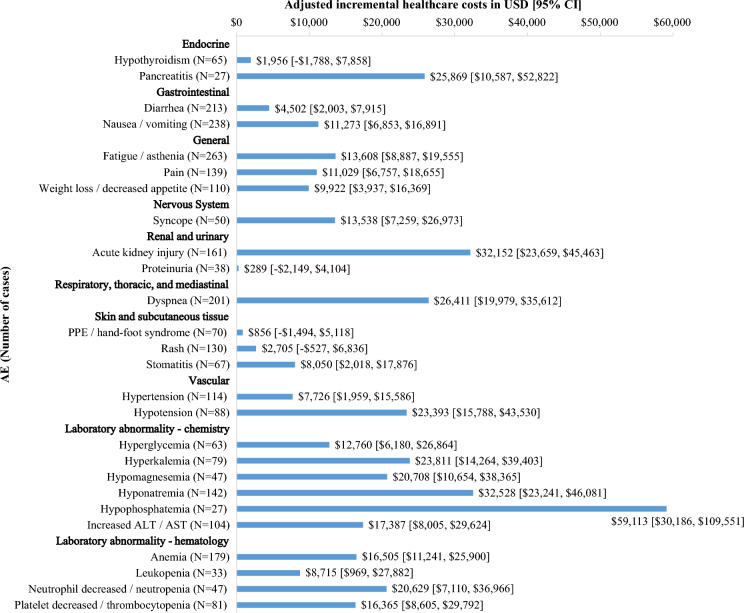
Results: The study included 1681 patients with aRCC (mean [standard deviation; SD] age, 60.8 [10.6] years; 73.1% male), of which 1542 (91.7%) had at least one AE. AEs were mostly diagnosed in the outpatient (OP) setting. For most AEs, cases had significantly higher unadjusted and adjusted costs than controls. Costs associated with AEs ranged from < 300 US dollars (USD) for proteinuria to nearly 60,000 USD for hypophosphatemia. Seventeen AEs had adjusted 30-day costs exceeding 10,000 USD; of these, nine (pancreatitis, acute kidney injury, dyspnea, hypotension, hyperkalemia, hypomagnesemia, hyponatremia, hypophosphatemia, and neutrophil decreased/neutropenia) had 30-day costs exceeding 20,000 USD.
Limitations: The study was subject to limitations of all observational analyses of claims data (e.g., residual confounding). Observed cost differences may not have been solely attributable to an AE of interest. Study findings may not be generalizable to aRCC patient populations outside the USA.
Conclusion: Most patients experienced at least one AE after initiation of first-line treatment with a TKI or combination therapies of TKIs and immunotherapy. There were substantial costs associated with AEs. Considering both safety and efficacy profiles when selecting optimal treatments can potentially mitigate healthcare costs for aRCC.
期刊介绍:
PharmacoEconomics - Open focuses on applied research on the economic implications and health outcomes associated with drugs, devices and other healthcare interventions. The journal includes, but is not limited to, the following research areas:Economic analysis of healthcare interventionsHealth outcomes researchCost-of-illness studiesQuality-of-life studiesAdditional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in PharmacoEconomics -Open may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.All manuscripts are subject to peer review by international experts. Letters to the Editor are welcomed and will be considered for publication.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
