Efficacy and safety of Advanced Combination Treatment in immune-mediated inflammatory disease: A systematic review and meta-analysis of randomized controlled trials
Virginia Solitano , Yuhong Yuan , Siddharth Singh , Christopher Ma , Olga Maria Nardone , Gionata Fiorino , Maria Laura Acosta Felquer , Lillian Barra , Maria-Antonietta D'Agostino , Janet Pope , Laurent Peyrin-Biroulet , Silvio Danese , Vipul Jairath
{"title":"Efficacy and safety of Advanced Combination Treatment in immune-mediated inflammatory disease: A systematic review and meta-analysis of randomized controlled trials","authors":"Virginia Solitano , Yuhong Yuan , Siddharth Singh , Christopher Ma , Olga Maria Nardone , Gionata Fiorino , Maria Laura Acosta Felquer , Lillian Barra , Maria-Antonietta D'Agostino , Janet Pope , Laurent Peyrin-Biroulet , Silvio Danese , Vipul Jairath","doi":"10.1016/j.jaut.2024.103331","DOIUrl":null,"url":null,"abstract":"<div><h3>Objectives</h3><div>Advanced combination treatment (ACT), defined as a combination of at least 2 biologic agents, a biologic agent and an oral small molecule, 2 oral small molecules drug with different mechanisms of action is a proposed strategy to improve outcomes in patients with immune-mediated inflammatory disease (IMID). We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) comparing ACT with monotherapy in patients with select IMIDs.</div></div><div><h3>Methods</h3><div>Through a systematic literature search, we identified 10 RCTs (n = 1154) comparing ACT with single agent therapy (monotherapy). The primary outcome was induction of clinical remission. Secondary outcomes were adverse events, serious adverse events, infections, and serious infections. We performed random-effects meta-analysis and used GRADE to appraise certainty of evidence.</div></div><div><h3>Results</h3><div>Eight out of 10 trials investigated an anti-TNF-α drug (e.g., etanercept, infliximab, golimumab, certolizumab) combined with another biologic (e.g anti-IL-23, anti-integrin, anti-IL-1) or an oral small molecule. There was no significant difference in the likelihood of achieving clinical remission with ACT vs. monotherapy in patients with rheumatoid arthritis (n = 7 RCTs) (RR, 1.75 [95 % CI 0.60–5.13]; moderate heterogeneity (I<sup>2</sup> = 33 %)] and systemic lupus erythematosus (n = 1) (RR, 1.20 [0.53–2.72]) (GRADE; low certainty evidence). Patients with rheumatoid arthritis in the ACT arm were more likely to experience adverse events (RR, 1.07 [1.01–1.12]) compared to monotherapy. ACT led to higher rates of induction of clinical remission in patients with IBD (n = 2 RCTs) (RR, 1.68 [1.15–2.46]) with minimal heterogeneity (I<sup>2</sup> = 15 %) (GRADE; low certainty evidence), and no differences in the likelihood of adverse events (RR 0.92 [0.80–1.05]). There were no differences in the risk of infections or serious infections in patients treated with ACT or monotherapy with rheumatological disease or IBD.</div></div><div><h3>Conclusions</h3><div>ACT did not offer clinical benefit in patients with rheumatological IMIDs and resulted in higher rate adverse events in rheumatoid arthritis. ACT may offer clinical benefit without a clear safety signal in patients with IBD, but further trials are warranted. The variability in ACT regimens across studies limits the generalizability of these findings.</div></div>","PeriodicalId":15245,"journal":{"name":"Journal of autoimmunity","volume":"149 ","pages":"Article 103331"},"PeriodicalIF":7.0000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of autoimmunity","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0896841124001653","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/6 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives
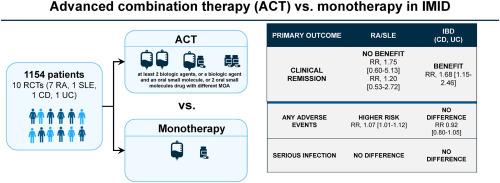
Advanced combination treatment (ACT), defined as a combination of at least 2 biologic agents, a biologic agent and an oral small molecule, 2 oral small molecules drug with different mechanisms of action is a proposed strategy to improve outcomes in patients with immune-mediated inflammatory disease (IMID). We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) comparing ACT with monotherapy in patients with select IMIDs.
Methods
Through a systematic literature search, we identified 10 RCTs (n = 1154) comparing ACT with single agent therapy (monotherapy). The primary outcome was induction of clinical remission. Secondary outcomes were adverse events, serious adverse events, infections, and serious infections. We performed random-effects meta-analysis and used GRADE to appraise certainty of evidence.
Results
Eight out of 10 trials investigated an anti-TNF-α drug (e.g., etanercept, infliximab, golimumab, certolizumab) combined with another biologic (e.g anti-IL-23, anti-integrin, anti-IL-1) or an oral small molecule. There was no significant difference in the likelihood of achieving clinical remission with ACT vs. monotherapy in patients with rheumatoid arthritis (n = 7 RCTs) (RR, 1.75 [95 % CI 0.60–5.13]; moderate heterogeneity (I2 = 33 %)] and systemic lupus erythematosus (n = 1) (RR, 1.20 [0.53–2.72]) (GRADE; low certainty evidence). Patients with rheumatoid arthritis in the ACT arm were more likely to experience adverse events (RR, 1.07 [1.01–1.12]) compared to monotherapy. ACT led to higher rates of induction of clinical remission in patients with IBD (n = 2 RCTs) (RR, 1.68 [1.15–2.46]) with minimal heterogeneity (I2 = 15 %) (GRADE; low certainty evidence), and no differences in the likelihood of adverse events (RR 0.92 [0.80–1.05]). There were no differences in the risk of infections or serious infections in patients treated with ACT or monotherapy with rheumatological disease or IBD.
Conclusions
ACT did not offer clinical benefit in patients with rheumatological IMIDs and resulted in higher rate adverse events in rheumatoid arthritis. ACT may offer clinical benefit without a clear safety signal in patients with IBD, but further trials are warranted. The variability in ACT regimens across studies limits the generalizability of these findings.
期刊介绍:
The Journal of Autoimmunity serves as the primary publication for research on various facets of autoimmunity. These include topics such as the mechanism of self-recognition, regulation of autoimmune responses, experimental autoimmune diseases, diagnostic tests for autoantibodies, as well as the epidemiology, pathophysiology, and treatment of autoimmune diseases. While the journal covers a wide range of subjects, it emphasizes papers exploring the genetic, molecular biology, and cellular aspects of the field.
The Journal of Translational Autoimmunity, on the other hand, is a subsidiary journal of the Journal of Autoimmunity. It focuses specifically on translating scientific discoveries in autoimmunity into clinical applications and practical solutions. By highlighting research that bridges the gap between basic science and clinical practice, the Journal of Translational Autoimmunity aims to advance the understanding and treatment of autoimmune diseases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
