Kelley Chan, Bryan E Palis, Joseph H Cotler, Lauren M Janczewski, Ronald J Weigel, David J Bentrem, Clifford Y Ko
{"title":"Association of commission on cancer accreditation with receipt of guideline-concordant care and survival among patients with colon cancer.","authors":"Kelley Chan, Bryan E Palis, Joseph H Cotler, Lauren M Janczewski, Ronald J Weigel, David J Bentrem, Clifford Y Ko","doi":"10.1002/wjs.12391","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Guideline-concordant care (GCC) is associated with improved survival for patients with cancer; however, variations in receipt of GCC remain a concern. The objective of this study was to evaluate the association of Commission on Cancer (CoC) hospital accreditation status with receipt of GCC and survival among patients with colon cancer.</p><p><strong>Methods: </strong>This retrospective observational study identified patients diagnosed with stage I-IV colon cancer from 2018 to 2020 from the National Program of Cancer Registries and Surveillance, Epidemiology, and End Results Program Database. Guideline concordance was defined as receipt of stage-appropriate lymphadenectomy or chemotherapy. Multivariable logistic regression models investigated associations with receipt of GCC. Cox proportional hazards regression models assessed 3-year cancer-specific mortality risk.</p><p><strong>Results: </strong>Of 222,583 patients with colon cancer, 146,629 (91.2%) of eligible patients received guideline-concordant lymphadenectomy and 70,586 (81.9%) of the eligible patients received guideline-concordant chemotherapy. Treatment at CoC-accredited hospitals was the strongest modifiable predictor for receipt of guideline-concordant lymphadenectomy (odds ratio [OR] 1.82; 95% confidence interval [CI] 1.75-1.88) and chemotherapy (OR 2.14; 95% CI 2.06-2.23). Among patients treated at CoC-accredited hospitals, risk adjusted mortality was decreased for patients with stage I-II disease (hazard ratio [HR] 0.94; 95% CI 0.80-0.99), stage III disease (HR 0.93; 95% CI 0.88-0.98), and stage IV disease (HR 0.88; 95% CI 0.84-0.92).</p><p><strong>Conclusions: </strong>For patients with colon cancer, treatment at CoC-accredited hospitals was associated with increased receipt of GCC and decreased mortality risk. Benchmarking data may serve as a valuable accountability tool for quality assessment to improve cancer treatment and outcomes.</p>","PeriodicalId":23926,"journal":{"name":"World Journal of Surgery","volume":" ","pages":"34-45"},"PeriodicalIF":2.2000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11711115/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/wjs.12391","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/7 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Guideline-concordant care (GCC) is associated with improved survival for patients with cancer; however, variations in receipt of GCC remain a concern. The objective of this study was to evaluate the association of Commission on Cancer (CoC) hospital accreditation status with receipt of GCC and survival among patients with colon cancer.
Methods: This retrospective observational study identified patients diagnosed with stage I-IV colon cancer from 2018 to 2020 from the National Program of Cancer Registries and Surveillance, Epidemiology, and End Results Program Database. Guideline concordance was defined as receipt of stage-appropriate lymphadenectomy or chemotherapy. Multivariable logistic regression models investigated associations with receipt of GCC. Cox proportional hazards regression models assessed 3-year cancer-specific mortality risk.
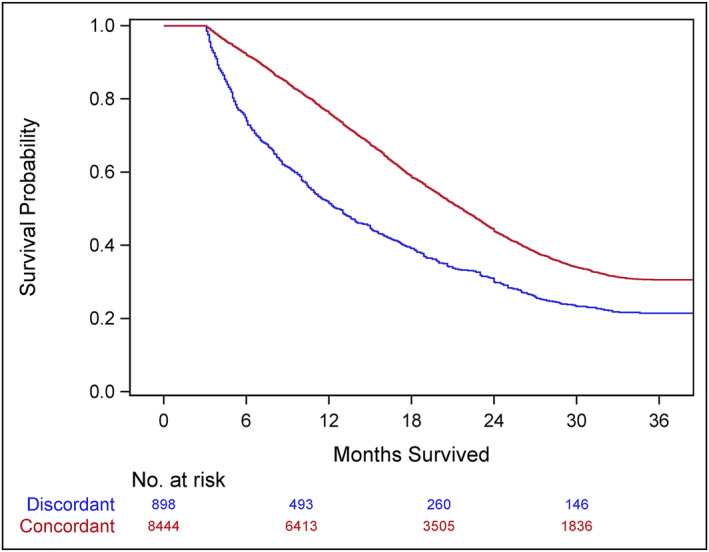
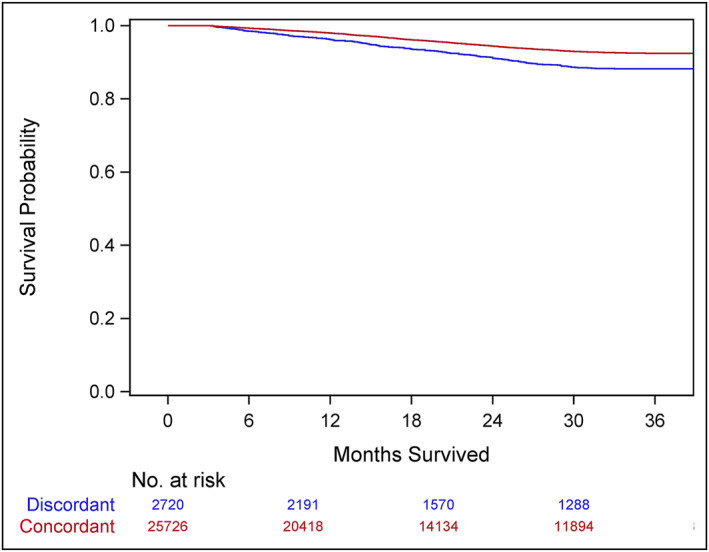
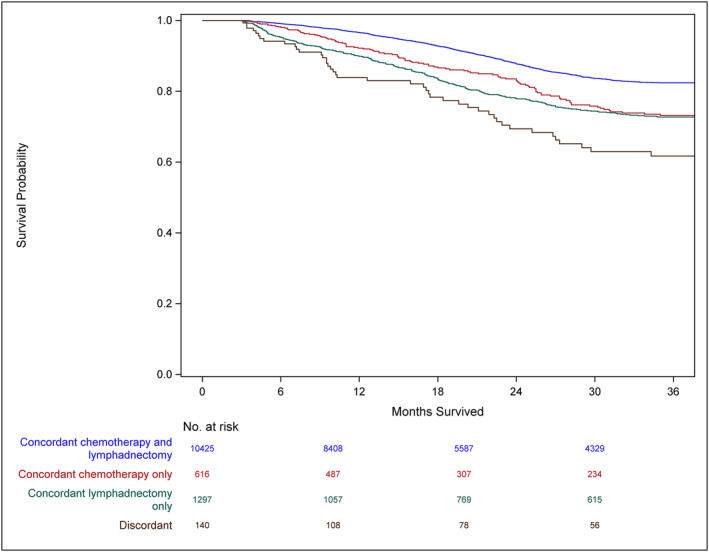
Results: Of 222,583 patients with colon cancer, 146,629 (91.2%) of eligible patients received guideline-concordant lymphadenectomy and 70,586 (81.9%) of the eligible patients received guideline-concordant chemotherapy. Treatment at CoC-accredited hospitals was the strongest modifiable predictor for receipt of guideline-concordant lymphadenectomy (odds ratio [OR] 1.82; 95% confidence interval [CI] 1.75-1.88) and chemotherapy (OR 2.14; 95% CI 2.06-2.23). Among patients treated at CoC-accredited hospitals, risk adjusted mortality was decreased for patients with stage I-II disease (hazard ratio [HR] 0.94; 95% CI 0.80-0.99), stage III disease (HR 0.93; 95% CI 0.88-0.98), and stage IV disease (HR 0.88; 95% CI 0.84-0.92).
Conclusions: For patients with colon cancer, treatment at CoC-accredited hospitals was associated with increased receipt of GCC and decreased mortality risk. Benchmarking data may serve as a valuable accountability tool for quality assessment to improve cancer treatment and outcomes.
期刊介绍:
World Journal of Surgery is the official publication of the International Society of Surgery/Societe Internationale de Chirurgie (iss-sic.com). Under the editorship of Dr. Julie Ann Sosa, World Journal of Surgery provides an in-depth, international forum for the most authoritative information on major clinical problems in the fields of clinical and experimental surgery, surgical education, and socioeconomic aspects of surgical care. Contributions are reviewed and selected by a group of distinguished surgeons from across the world who make up the Editorial Board.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
