Feasibility and accuracy of pediatric core temperature measurement using an esophageal probe inserted through the gastric lumen of a second-generation supraglottic airway device: a prospective observational study.
Yeon-Ju Kim, Eundong Lee, Jaedo Lee, Hyungtae Kim, Won Uk Koh, Young-Jin Ro, Ha-Jung Kim
{"title":"Feasibility and accuracy of pediatric core temperature measurement using an esophageal probe inserted through the gastric lumen of a second-generation supraglottic airway device: a prospective observational study.","authors":"Yeon-Ju Kim, Eundong Lee, Jaedo Lee, Hyungtae Kim, Won Uk Koh, Young-Jin Ro, Ha-Jung Kim","doi":"10.17085/apm.23150","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Accurate core temperature measurement in children is crucial; however, measuring esophageal temperature (TE) using a supraglottic airway device (SAD) can be challenging. Second-generation SADs, which have a gastric channel, can measure TE, and reduce gastric air volume. This study aimed to compare TE, measured using a probe inserted through the SAD gastric channel, with tympanic membrane (TTM) and forehead (TZHF) temperatures, measured using a zero-heat-flux cutaneous thermometer, with rectal temperature (TR).</p><p><strong>Methods: </strong>Temperature was recorded at 10-min intervals from 10 min after probe insertion until completion of surgery. We performed an equivalence test to evaluate whether the TE, TTM, and TZHF were equivalent to TR, with a margin of 0.3°C. Additionally, intraclass correlation coefficients (ICC) were calculated to assess the reliability of TE and TR at each time point.</p><p><strong>Results: </strong>We included 41 patients in the final analysis. In all patients, the esophageal probe was successfully inserted through the gastric channel of the SAD. When assessing agreement with TR as a reference, TE demonstrated equivalent results at all time points (P < 0.001 at 0, 10, 20, 30, and 40-min intervals and P = 0.018 at the 50-min interval), except at the completion of surgery (P = 0.697). TE also demonstrated good reliability with TR as a reference throughout the surgery (ICC > 0.75).</p><p><strong>Conclusions: </strong>In children with SAD insertion, TE can be accurately and feasibly measured through the SAD's gastric channel, making it suitable for routine application.</p>","PeriodicalId":101360,"journal":{"name":"Anesthesia and pain medicine","volume":"19 Suppl 1","pages":"S105-S112"},"PeriodicalIF":3.2000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11566552/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesia and pain medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17085/apm.23150","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/28 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
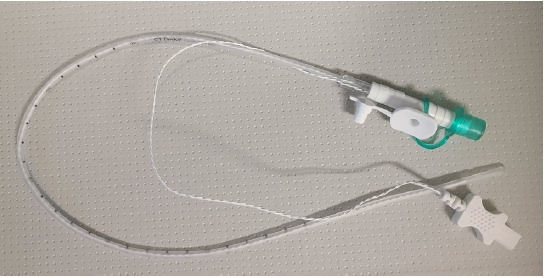
Background: Accurate core temperature measurement in children is crucial; however, measuring esophageal temperature (TE) using a supraglottic airway device (SAD) can be challenging. Second-generation SADs, which have a gastric channel, can measure TE, and reduce gastric air volume. This study aimed to compare TE, measured using a probe inserted through the SAD gastric channel, with tympanic membrane (TTM) and forehead (TZHF) temperatures, measured using a zero-heat-flux cutaneous thermometer, with rectal temperature (TR).
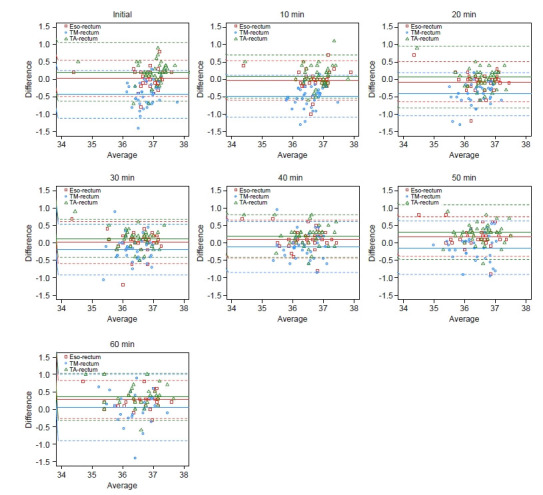
Methods: Temperature was recorded at 10-min intervals from 10 min after probe insertion until completion of surgery. We performed an equivalence test to evaluate whether the TE, TTM, and TZHF were equivalent to TR, with a margin of 0.3°C. Additionally, intraclass correlation coefficients (ICC) were calculated to assess the reliability of TE and TR at each time point.
Results: We included 41 patients in the final analysis. In all patients, the esophageal probe was successfully inserted through the gastric channel of the SAD. When assessing agreement with TR as a reference, TE demonstrated equivalent results at all time points (P < 0.001 at 0, 10, 20, 30, and 40-min intervals and P = 0.018 at the 50-min interval), except at the completion of surgery (P = 0.697). TE also demonstrated good reliability with TR as a reference throughout the surgery (ICC > 0.75).
Conclusions: In children with SAD insertion, TE can be accurately and feasibly measured through the SAD's gastric channel, making it suitable for routine application.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
