Stephan A C Schoonvelde, Isabell Wiethoff, Peter-Paul Zwetsloot, Alexander Hirsch, Christian Knackstedt, Tjeerd Germans, Maurits Sikking, Arend F L Schinkel, Marjon A van Slegtenhorst, Judith M A Verhagen, Rudolf A de Boer, Silvia M A A Evers, Mickaël Hiligsmann, Michelle Michels
{"title":"Loss of quality of life and increased societal costs in patients with hypertrophic cardiomyopathy: the AFFECT-HCM study.","authors":"Stephan A C Schoonvelde, Isabell Wiethoff, Peter-Paul Zwetsloot, Alexander Hirsch, Christian Knackstedt, Tjeerd Germans, Maurits Sikking, Arend F L Schinkel, Marjon A van Slegtenhorst, Judith M A Verhagen, Rudolf A de Boer, Silvia M A A Evers, Mickaël Hiligsmann, Michelle Michels","doi":"10.1093/ehjqcco/qcae092","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Hypertrophic cardiomyopathy (HCM) is the most prevalent inherited cardiac disease. The impact of HCM on quality of life (QoL) and societal costs remains poorly understood. This prospective multi-centre burden of disease study estimated QoL and societal costs of genotyped HCM patients and genotype-positive phenotype-negative (G+/P-) subjects.</p><p><strong>Methods and results: </strong>Participants were categorized into three groups based on genotype and phenotype: (i) G+/P- [left ventricular (LV) wall thickness <13 mm], (ii) non-obstructive HCM [nHCM, LV outflow tract (LVOT) gradient <30 mmHg], and (iii) obstructive HCM (oHCM, LVOT gradient ≥30 mmHg). We assessed QoL with EQ-5D-5L and Kansas City Cardiomyopathy Questionnaires (KCCQ). Societal costs were measured using medical consumption (Medical Consumption Questionnaire) and productivity cost (iMTA Productivity Cost Questionnaire) questionnaires. We performed subanalyses within three age groups: <40, 40-59, and ≥60 years. From three Dutch hospitals, 506 subjects were enrolled (84 G+/P-, 313 nHCM, 109 oHCM; median age 59 years, 39% female). HCM (both nHCM and oHCM) patients reported reduced QoL vs. G+/P- subjects (KCCQ: 88 vs. 98, EQ-5D-5L: 0.88 vs. 0.96; both P < 0.001). oHCM patients reported lower KCCQ scores than nHCM patients (83 vs. 89, P = 0.036). Societal costs were significantly higher in HCM patients (€19,035/year vs. €7385/year) compared with G+/P- controls, mainly explained by higher healthcare costs and productivity losses. Being symptomatic and of younger age (<60 years) particularly led to decreased QoL and increased costs.</p><p><strong>Conclusion: </strong>HCM is associated with decreased QoL and increased societal costs, especially in younger and symptomatic patients. oHCM patients were more frequently symptomatic than nHCM patients. This study highlights the substantial disease burden of HCM and can aid in assessing new therapy cost-effectiveness for HCM in the future.</p>","PeriodicalId":11869,"journal":{"name":"European Heart Journal - Quality of Care and Clinical Outcomes","volume":" ","pages":"174-185"},"PeriodicalIF":4.6000,"publicationDate":"2025-03-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11879321/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal - Quality of Care and Clinical Outcomes","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ehjqcco/qcae092","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Hypertrophic cardiomyopathy (HCM) is the most prevalent inherited cardiac disease. The impact of HCM on quality of life (QoL) and societal costs remains poorly understood. This prospective multi-centre burden of disease study estimated QoL and societal costs of genotyped HCM patients and genotype-positive phenotype-negative (G+/P-) subjects.
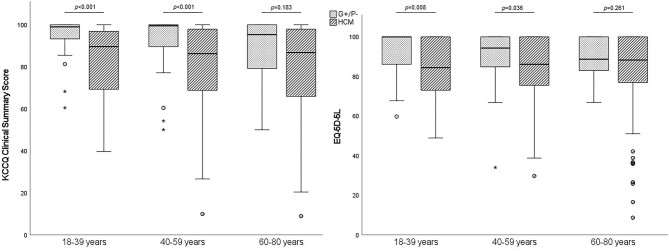
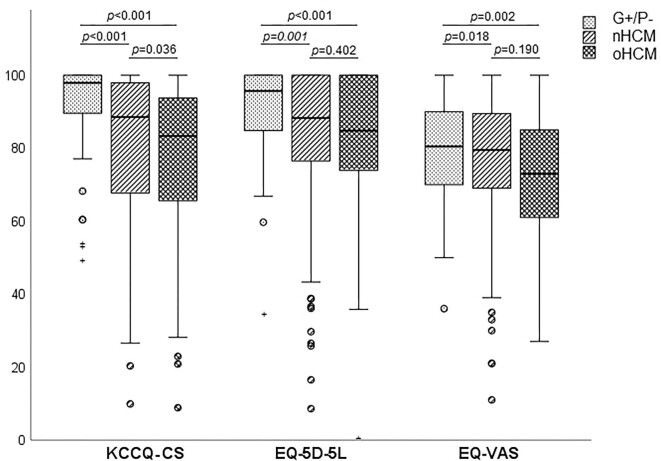
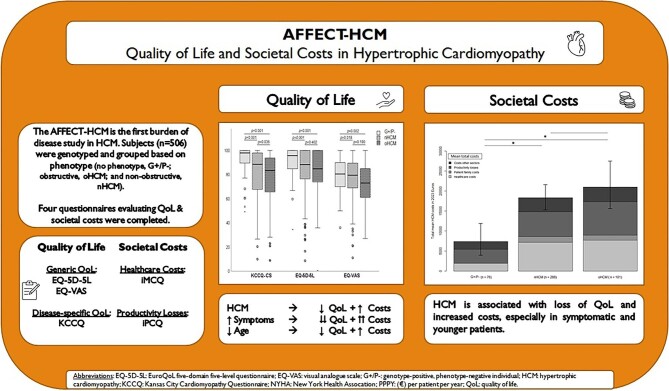
Methods and results: Participants were categorized into three groups based on genotype and phenotype: (i) G+/P- [left ventricular (LV) wall thickness <13 mm], (ii) non-obstructive HCM [nHCM, LV outflow tract (LVOT) gradient <30 mmHg], and (iii) obstructive HCM (oHCM, LVOT gradient ≥30 mmHg). We assessed QoL with EQ-5D-5L and Kansas City Cardiomyopathy Questionnaires (KCCQ). Societal costs were measured using medical consumption (Medical Consumption Questionnaire) and productivity cost (iMTA Productivity Cost Questionnaire) questionnaires. We performed subanalyses within three age groups: <40, 40-59, and ≥60 years. From three Dutch hospitals, 506 subjects were enrolled (84 G+/P-, 313 nHCM, 109 oHCM; median age 59 years, 39% female). HCM (both nHCM and oHCM) patients reported reduced QoL vs. G+/P- subjects (KCCQ: 88 vs. 98, EQ-5D-5L: 0.88 vs. 0.96; both P < 0.001). oHCM patients reported lower KCCQ scores than nHCM patients (83 vs. 89, P = 0.036). Societal costs were significantly higher in HCM patients (€19,035/year vs. €7385/year) compared with G+/P- controls, mainly explained by higher healthcare costs and productivity losses. Being symptomatic and of younger age (<60 years) particularly led to decreased QoL and increased costs.
Conclusion: HCM is associated with decreased QoL and increased societal costs, especially in younger and symptomatic patients. oHCM patients were more frequently symptomatic than nHCM patients. This study highlights the substantial disease burden of HCM and can aid in assessing new therapy cost-effectiveness for HCM in the future.
期刊介绍:
European Heart Journal - Quality of Care & Clinical Outcomes is an English language, peer-reviewed journal dedicated to publishing cardiovascular outcomes research. It serves as an official journal of the European Society of Cardiology and maintains a close alliance with the European Heart Health Institute. The journal disseminates original research and topical reviews contributed by health scientists globally, with a focus on the quality of care and its impact on cardiovascular outcomes at the hospital, national, and international levels. It provides a platform for presenting the most outstanding cardiovascular outcomes research to influence cardiovascular public health policy on a global scale. Additionally, the journal aims to motivate young investigators and foster the growth of the outcomes research community.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
