Predictive Factors of Unexpected Hospitalization within Six Months of Undergoing Percutaneous Coronary Intervention in Patients with Chronic Coronary Disease.
{"title":"Predictive Factors of Unexpected Hospitalization within Six Months of Undergoing Percutaneous Coronary Intervention in Patients with Chronic Coronary Disease.","authors":"Tetsuo Furukawa, Isamu Mizote, Tatsuya Shiraki, Daisuke Nakamura, Mayu Nishio, Naoki Fukushima, Takashi Kitao, Kensuke Yokoi, Masahiro Kumada, Motoaki Kitagawa, Kunihiko Nagai, Kiyoshi Kume, Keiji Hirooka, Tsutomu Nakagawa, Tohru Ohama, Mitsuyoshi Takahara, Shungo Hikoso, Yasushi Sakata","doi":"10.2169/internalmedicine.3929-24","DOIUrl":null,"url":null,"abstract":"<p><p>Objective Recent guidelines recommend dual antiplatelet therapy (DAPT) for six months following percutaneous coronary intervention (PCI) in patients with chronic coronary disease, as unexpected hospitalization can trigger DAPT discontinuation. This study evaluated the predictive factors for unexpected hospitalization within six months after PCI in patients with chronic coronary disease. Methods This prospective multicenter study included 412 patients who underwent PCI for chronic coronary disease. Unexpected hospitalization was defined as a prolonged hospital stay, unscheduled readmission, and all-cause mortality. The predictive factors for unexpected hospitalization within six months post-PCI were evaluated using the Cox regression model. Results The rate of unexpected hospitalization 6 months after PCI was 10.8%±1.5%. Unexpected hospitalizations due to bleeding events accounted for 12.1% (n=5/41), whereas non-bleeding readmissions accounted for 87.9% (n=36/41). A multivariable analysis revealed that the number of Academic Research Consortium for High Bleeding Risk (ARC-HBR) major criteria met [adjusted hazard ratio (HR), 1.55; 95% confidence interval (CI), 1.05-2.29; p=0.026], body weight (adjusted HR, 2.44; 95% CI 1.33-4.49; p=0.004), and presence of diabetes mellitus (adjusted HR, 1.94; 95% CI 1.09-3.47; p=0.025) were independent risk factors for unexpected hospitalization. Among the major ARC-HBR criteria, oral anticoagulant use (adjusted HR, 2.39; 95% CI, 1.14-5.02, p=0.021) and active malignancy (adjusted HR, 3.85; 95% CI, 1.47-10.05; p=0.006) were significantly associated with unexpected hospitalization after adjusting for a low body weight and diabetes mellitus. Conclusions The majority of unexpected hospitalizations after PCI in patients with chronic coronary disease are attributed to non-bleeding causes. The assessment using major ARC-HBR criteria in these patients not only addresses bleeding risks but also underscores its predictive value in conjunction with a low body weight and diabetes mellitus for the prediction of unexpected hospitalization.</p>","PeriodicalId":13719,"journal":{"name":"Internal Medicine","volume":" ","pages":"1640-1647"},"PeriodicalIF":1.1000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12222949/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Internal Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2169/internalmedicine.3929-24","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/8 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
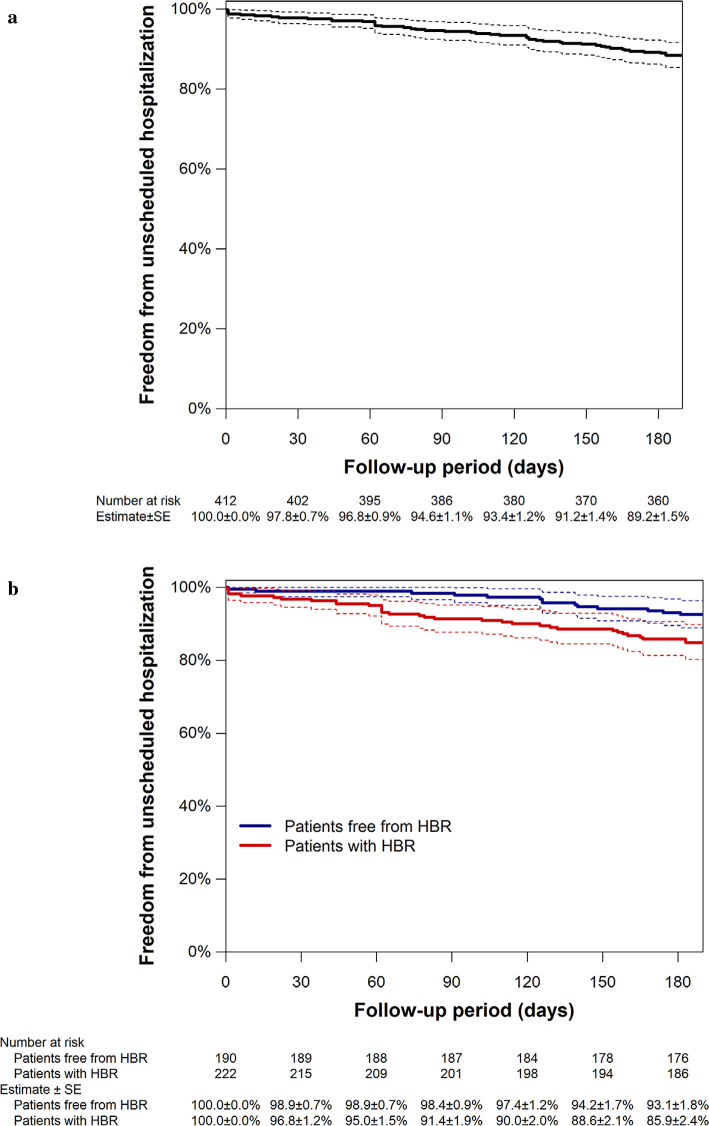
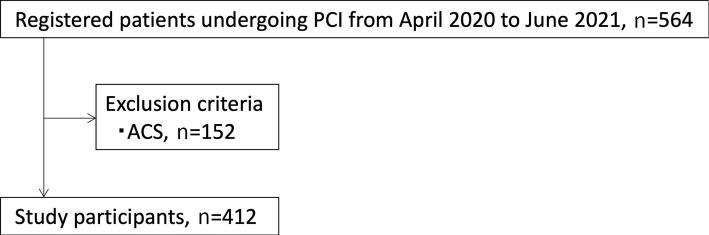
Objective Recent guidelines recommend dual antiplatelet therapy (DAPT) for six months following percutaneous coronary intervention (PCI) in patients with chronic coronary disease, as unexpected hospitalization can trigger DAPT discontinuation. This study evaluated the predictive factors for unexpected hospitalization within six months after PCI in patients with chronic coronary disease. Methods This prospective multicenter study included 412 patients who underwent PCI for chronic coronary disease. Unexpected hospitalization was defined as a prolonged hospital stay, unscheduled readmission, and all-cause mortality. The predictive factors for unexpected hospitalization within six months post-PCI were evaluated using the Cox regression model. Results The rate of unexpected hospitalization 6 months after PCI was 10.8%±1.5%. Unexpected hospitalizations due to bleeding events accounted for 12.1% (n=5/41), whereas non-bleeding readmissions accounted for 87.9% (n=36/41). A multivariable analysis revealed that the number of Academic Research Consortium for High Bleeding Risk (ARC-HBR) major criteria met [adjusted hazard ratio (HR), 1.55; 95% confidence interval (CI), 1.05-2.29; p=0.026], body weight (adjusted HR, 2.44; 95% CI 1.33-4.49; p=0.004), and presence of diabetes mellitus (adjusted HR, 1.94; 95% CI 1.09-3.47; p=0.025) were independent risk factors for unexpected hospitalization. Among the major ARC-HBR criteria, oral anticoagulant use (adjusted HR, 2.39; 95% CI, 1.14-5.02, p=0.021) and active malignancy (adjusted HR, 3.85; 95% CI, 1.47-10.05; p=0.006) were significantly associated with unexpected hospitalization after adjusting for a low body weight and diabetes mellitus. Conclusions The majority of unexpected hospitalizations after PCI in patients with chronic coronary disease are attributed to non-bleeding causes. The assessment using major ARC-HBR criteria in these patients not only addresses bleeding risks but also underscores its predictive value in conjunction with a low body weight and diabetes mellitus for the prediction of unexpected hospitalization.
期刊介绍:
Internal Medicine is an open-access online only journal published monthly by the Japanese Society of Internal Medicine.
Articles must be prepared in accordance with "The Uniform Requirements for Manuscripts Submitted to Biomedical Journals (see Annals of Internal Medicine 108: 258-265, 1988), must be contributed solely to the Internal Medicine, and become the property of the Japanese Society of Internal Medicine. Statements contained therein are the responsibility of the author(s). The Society reserves copyright and renewal on all published material and such material may not be reproduced in any form without the written permission of the Society.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
