Collaborative Care to Improve Quality of Life for Anxiety and Depression in Posttraumatic Epilepsy (CoCarePTE): Protocol for a Randomized Hybrid Effectiveness-Implementation Trial.
Heidi M Munger Clary, Beverly M Snively, Christian Cagle, Richard Kennerly, James N Kimball, Halley B Alexander, Gretchen A Brenes, Justin B Moore, Robin A Hurley
{"title":"Collaborative Care to Improve Quality of Life for Anxiety and Depression in Posttraumatic Epilepsy (CoCarePTE): Protocol for a Randomized Hybrid Effectiveness-Implementation Trial.","authors":"Heidi M Munger Clary, Beverly M Snively, Christian Cagle, Richard Kennerly, James N Kimball, Halley B Alexander, Gretchen A Brenes, Justin B Moore, Robin A Hurley","doi":"10.2196/59329","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Anxiety and depression in people with epilepsy are common and associated with poor outcomes; yet, they often go untreated due to poor mental health specialist access. Collaborative care is an integrated care model with a strong evidence base in primary care and medical settings, but it has not been evaluated in neurology clinics. Evaluating implementation outcomes when translating evidence-based interventions to new clinical settings to inform future scaling and incorporation into real-world practice is important.</p><p><strong>Objective: </strong>The Collaborative Care for Posttraumatic Epilepsy (CoCarePTE) trial aims to evaluate the effectiveness (improvement in emotional quality of life) and implementation of a collaborative care intervention for people with anxiety or depressive symptoms and posttraumatic epilepsy.</p><p><strong>Methods: </strong>CoCarePTE is a 2-site, randomized, single-blind, hybrid type 1 effectiveness-implementation trial that will randomize 60 adults to receive either neurology-based collaborative care or usual care. Adults receiving neurological care at participating centers with anxiety or depressive symptoms and a history of at least mild traumatic brain injury before epilepsy onset will be enrolled. The collaborative care intervention is a 24-week stepped-care model with video or telephone calls every 2 weeks by a care manager for measurement-based anxiety and depression care, seizure care monitoring, and brief therapy intervention delivery. This is supplemented by antidepressant prescribing recommendations by psychiatrists for neurologists via case conferences and care manager-facilitated team communication. In step 2 of the intervention, individuals with <50% symptom reduction by 10 weeks will receive an added 8-session remote cognitive behavioral therapy program. The study is powered to detect a moderate improvement in emotional quality of life. As a hybrid type 1 trial, effectiveness is the primary focus, with the primary outcome being a change in emotional quality of life at 6 months in the intervention group compared to control. Secondary effectiveness outcomes are 6-month changes in depression, anxiety, and overall quality of life. Implementation outcomes, including fidelity, acceptability, feasibility, and appropriateness, are evaluated before implementation and at 3 months. The primary effectiveness analysis will compare changes in emotional quality of life scores from baseline to 6 months between the intervention and control arms using multiple linear regression modeling, adjusting for study site and using an intent-to-treat approach.</p><p><strong>Results: </strong>Enrollment commenced in 2023, with modifications in the inclusion and exclusion made after the first 6 enrollees due to slow recruitment. Enrollment is expected to continue at least into early 2025.</p><p><strong>Conclusions: </strong>The CoCarePTE trial is novel in its use of a hybrid effectiveness-implementation design to evaluate an evidence-based mental health intervention in epilepsy, and by incorporating seizure care into a collaborative care model. If a significant improvement in emotional quality of life is found in the intervention group compared to usual care, this would support next step scaling or clinical implementation.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov NCT05353452; https://www.clinicaltrials.gov/study/NCT05353452.</p><p><strong>International registered report identifier (irrid): </strong>DERR1-10.2196/59329.</p>","PeriodicalId":14755,"journal":{"name":"JMIR Research Protocols","volume":"13 ","pages":"e59329"},"PeriodicalIF":1.5000,"publicationDate":"2024-11-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11602765/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Research Protocols","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/59329","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Anxiety and depression in people with epilepsy are common and associated with poor outcomes; yet, they often go untreated due to poor mental health specialist access. Collaborative care is an integrated care model with a strong evidence base in primary care and medical settings, but it has not been evaluated in neurology clinics. Evaluating implementation outcomes when translating evidence-based interventions to new clinical settings to inform future scaling and incorporation into real-world practice is important.
Objective: The Collaborative Care for Posttraumatic Epilepsy (CoCarePTE) trial aims to evaluate the effectiveness (improvement in emotional quality of life) and implementation of a collaborative care intervention for people with anxiety or depressive symptoms and posttraumatic epilepsy.
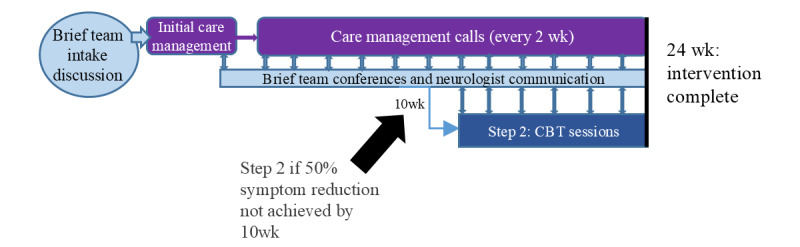
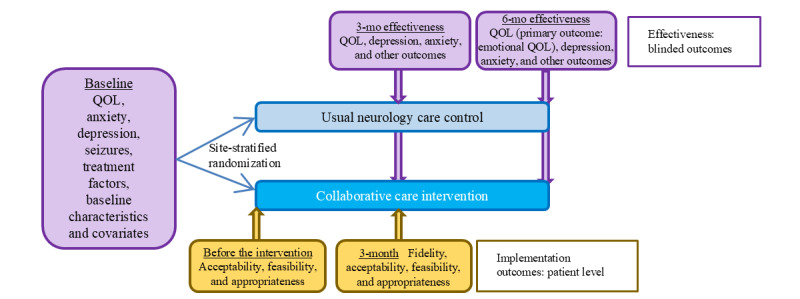
Methods: CoCarePTE is a 2-site, randomized, single-blind, hybrid type 1 effectiveness-implementation trial that will randomize 60 adults to receive either neurology-based collaborative care or usual care. Adults receiving neurological care at participating centers with anxiety or depressive symptoms and a history of at least mild traumatic brain injury before epilepsy onset will be enrolled. The collaborative care intervention is a 24-week stepped-care model with video or telephone calls every 2 weeks by a care manager for measurement-based anxiety and depression care, seizure care monitoring, and brief therapy intervention delivery. This is supplemented by antidepressant prescribing recommendations by psychiatrists for neurologists via case conferences and care manager-facilitated team communication. In step 2 of the intervention, individuals with <50% symptom reduction by 10 weeks will receive an added 8-session remote cognitive behavioral therapy program. The study is powered to detect a moderate improvement in emotional quality of life. As a hybrid type 1 trial, effectiveness is the primary focus, with the primary outcome being a change in emotional quality of life at 6 months in the intervention group compared to control. Secondary effectiveness outcomes are 6-month changes in depression, anxiety, and overall quality of life. Implementation outcomes, including fidelity, acceptability, feasibility, and appropriateness, are evaluated before implementation and at 3 months. The primary effectiveness analysis will compare changes in emotional quality of life scores from baseline to 6 months between the intervention and control arms using multiple linear regression modeling, adjusting for study site and using an intent-to-treat approach.
Results: Enrollment commenced in 2023, with modifications in the inclusion and exclusion made after the first 6 enrollees due to slow recruitment. Enrollment is expected to continue at least into early 2025.
Conclusions: The CoCarePTE trial is novel in its use of a hybrid effectiveness-implementation design to evaluate an evidence-based mental health intervention in epilepsy, and by incorporating seizure care into a collaborative care model. If a significant improvement in emotional quality of life is found in the intervention group compared to usual care, this would support next step scaling or clinical implementation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
